Downloaded 554 times
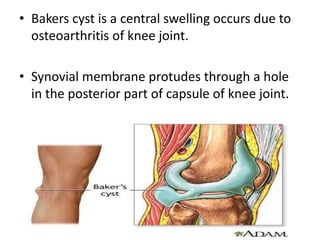
![4)the subcutaneous
[or superficial]
infrapatellar
bursa between
the patellar
ligament and skin.
5)the pretibial
bursa between
the tibial
tuberosity and
the skin. It allows
for movement of
the skin over the
tibial tuberosity.](https://image.slidesharecdn.com/jointsoflowerlimb-150916071225-lva1-app6891/85/Joints-of-lower-limb-32-320.jpg)
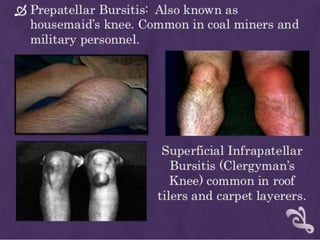
![Laterally there are four bursæ:
1) the lateral gastrocnemius [subtendinous]
bursa between the lateral head of
the gastrocnemius and the joint capsule
2) the fibular bursa between the lateral (fibular)
collateral ligament and the tendon of the biceps
femoris
3) the fibulopopliteal bursa between the fibular
collateral ligament and the tendon of
the popliteus
4) and the subpopliteal recess (or bursa) between
the tendon of the popliteus and the lateral
condyle of the femur](https://image.slidesharecdn.com/jointsoflowerlimb-150916071225-lva1-app6891/85/Joints-of-lower-limb-33-320.jpg)
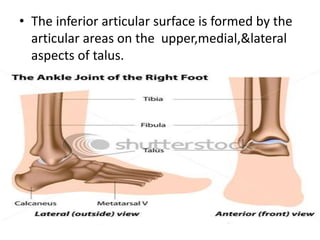
![Medially, there are five bursae:
1. the medial gastrocnemius [subtendinous]
bursa between the medial head of
the gastrocnemius and the joint capsule
2. the anserine bursa between the medial (tibial)
collateral ligament and the tendons of
the sartorius, gracilis, and semitendinosus (i.e. the pes
anserinus)
3. the bursa semimembranosa between the medial
collateral ligament and the tendon of
the semimembranosus
4. there is one between the tendon of the
semimembranosus and the head of the tibia
5. and occasionally there is a bursa between the tendons
of the semimembranosus and semitendinosus](https://image.slidesharecdn.com/jointsoflowerlimb-150916071225-lva1-app6891/85/Joints-of-lower-limb-34-320.jpg)





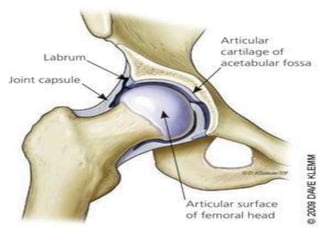
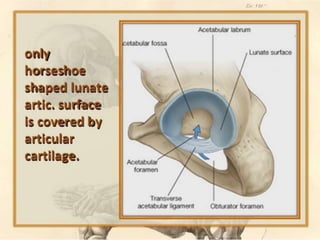
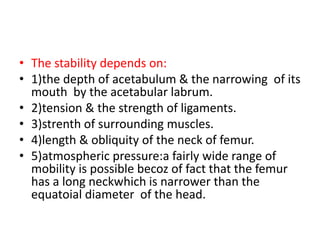
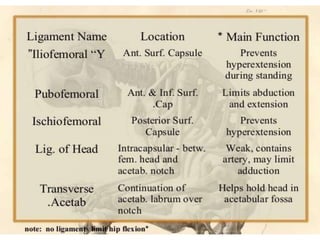
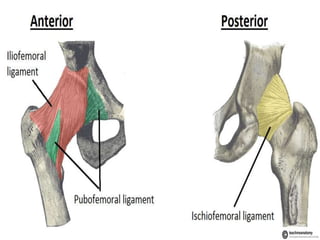
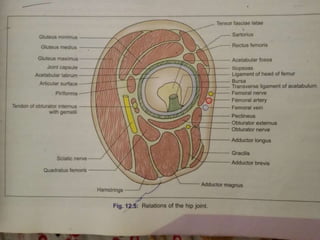
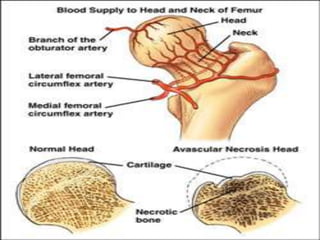
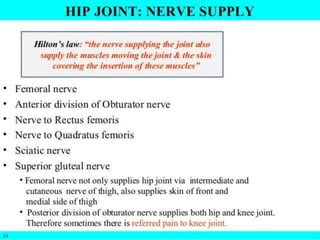
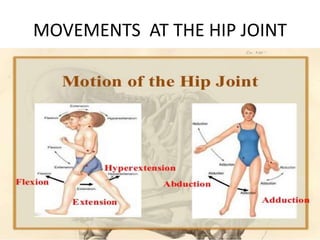
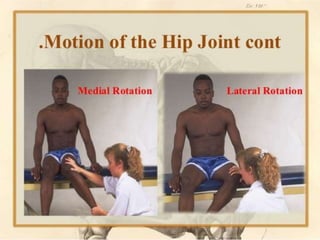
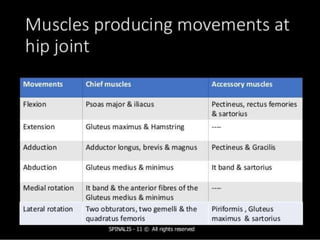
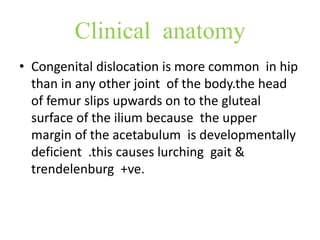
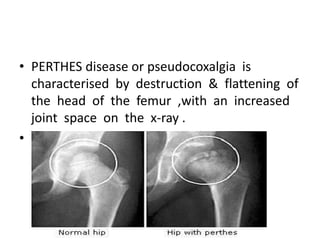
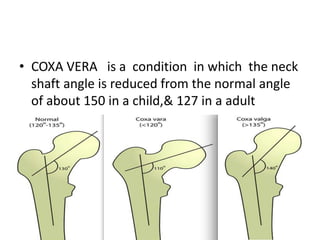
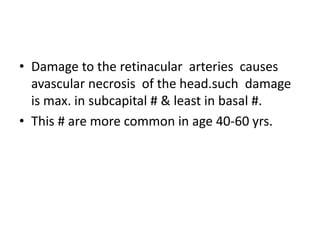
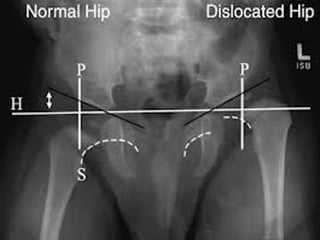
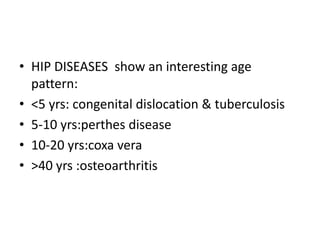
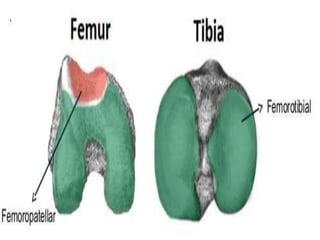
The document discusses the anatomy of the lower limb joints, including the hip, knee, and ankle joints. It describes the types of joints, articular surfaces, ligaments, movements, blood supply, clinical considerations, and gait for each joint. For the hip joint, it highlights the ball and socket construction, stability from muscles, ligaments and bone shape, and age-related diseases like osteoarthritis and fractures.



















































































