Downloaded 31 times

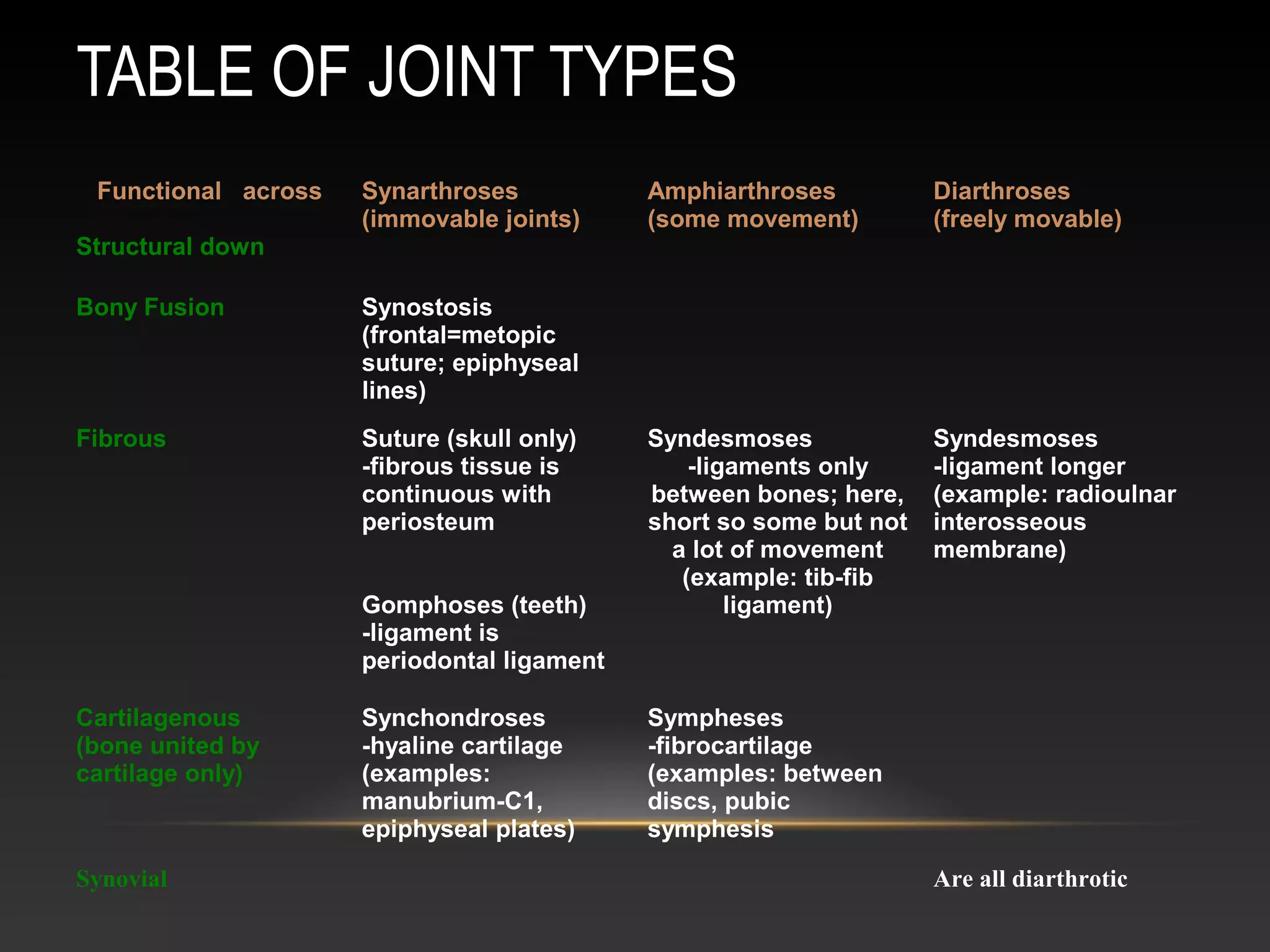



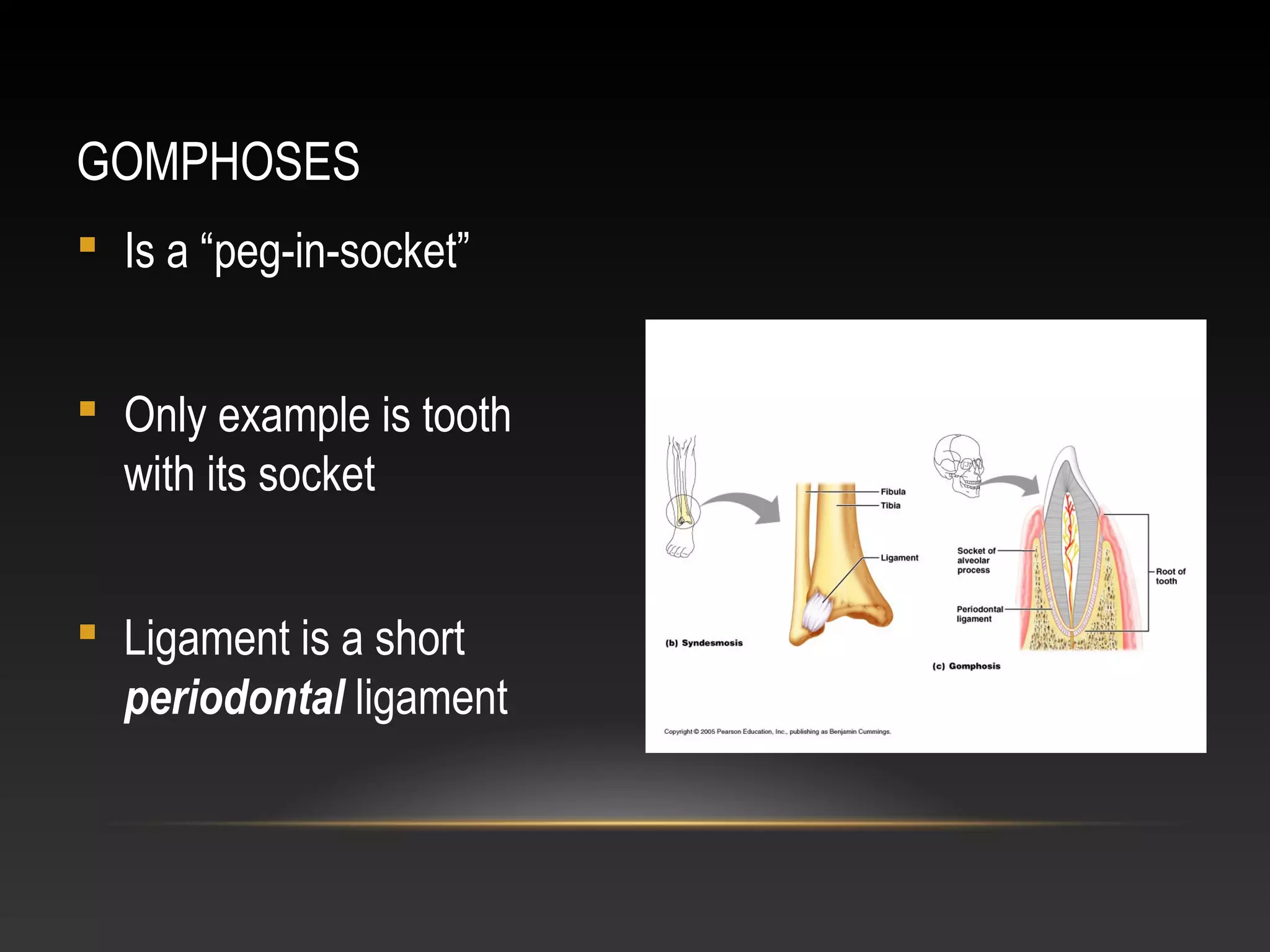



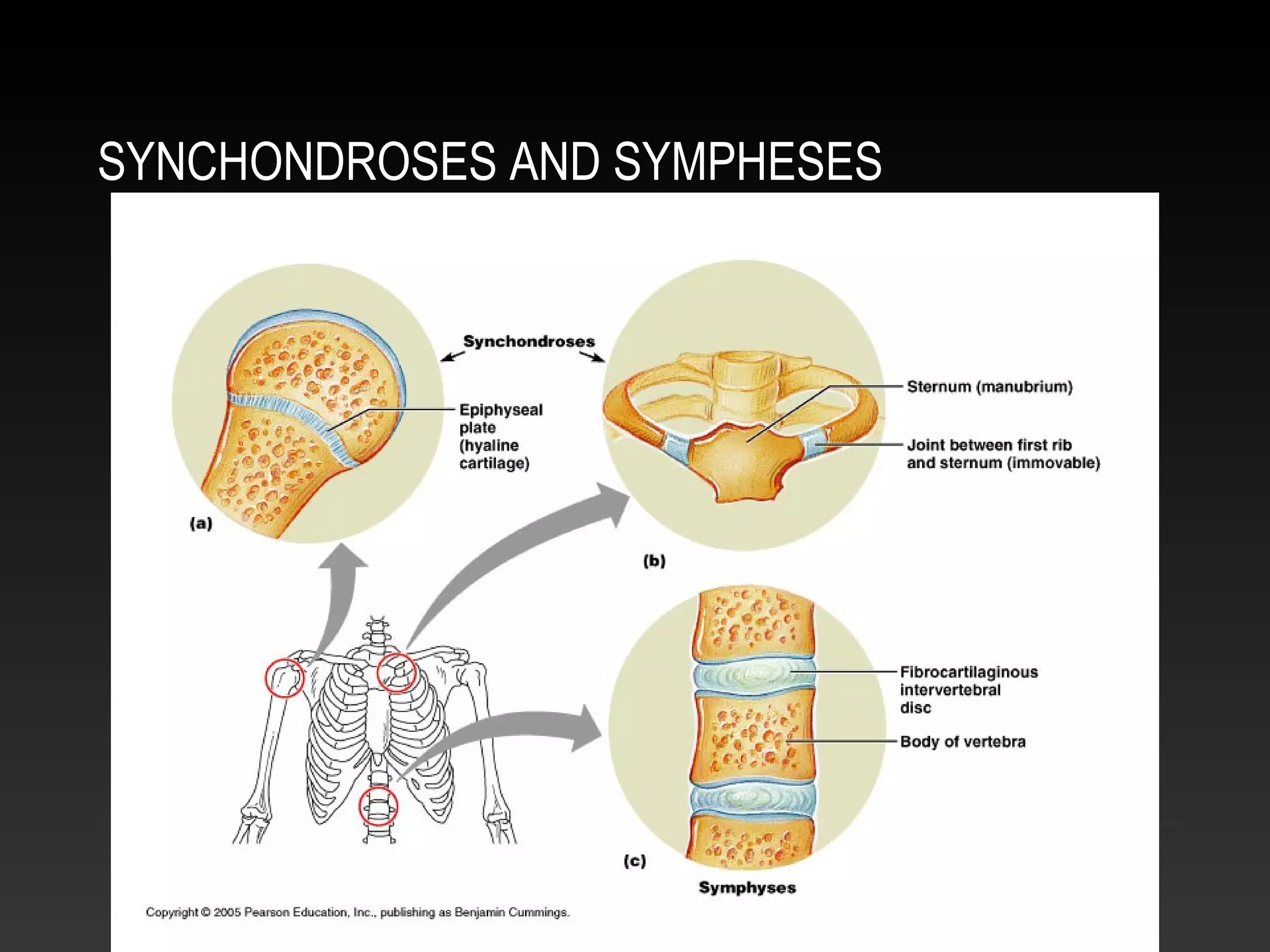
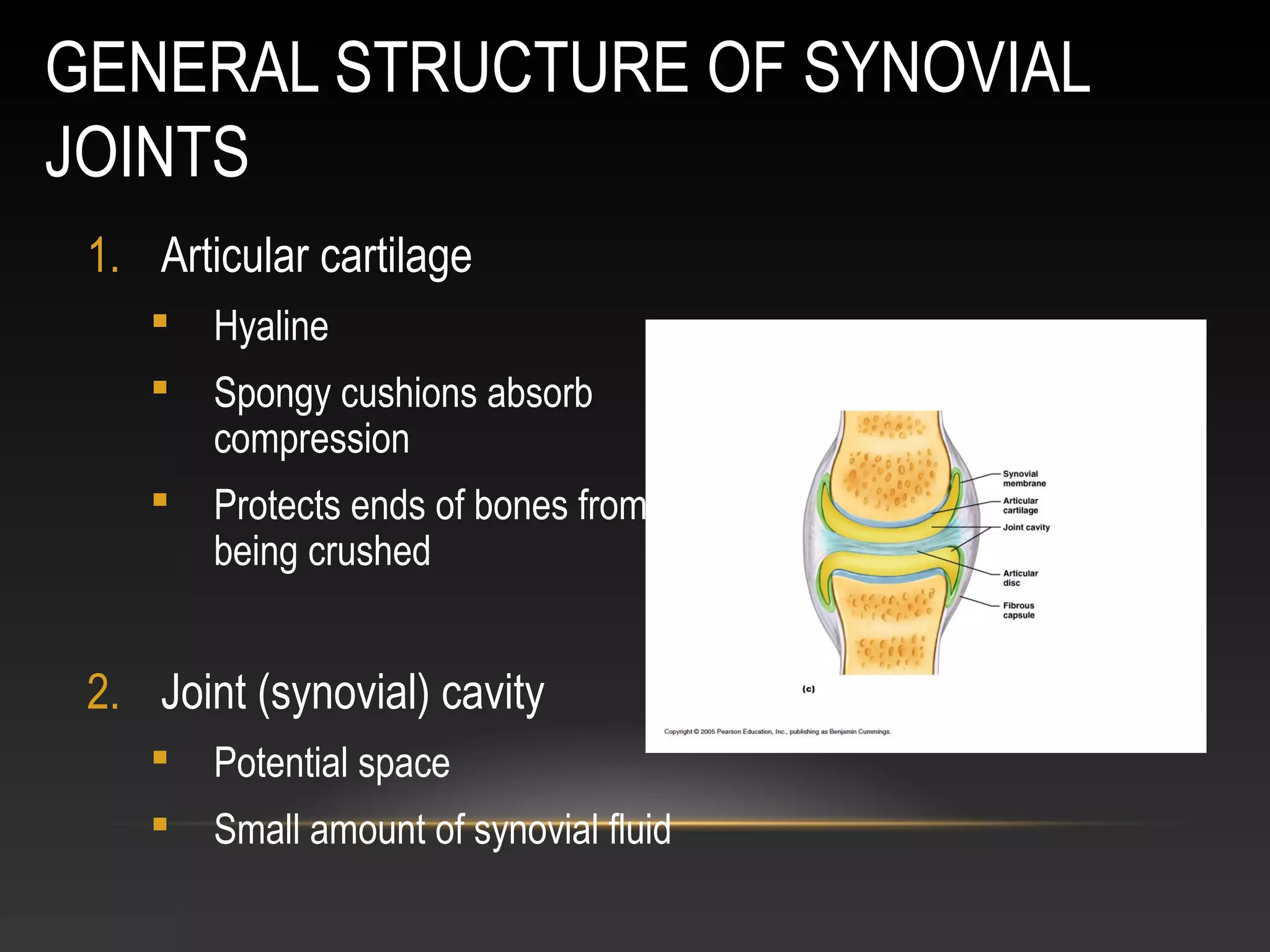
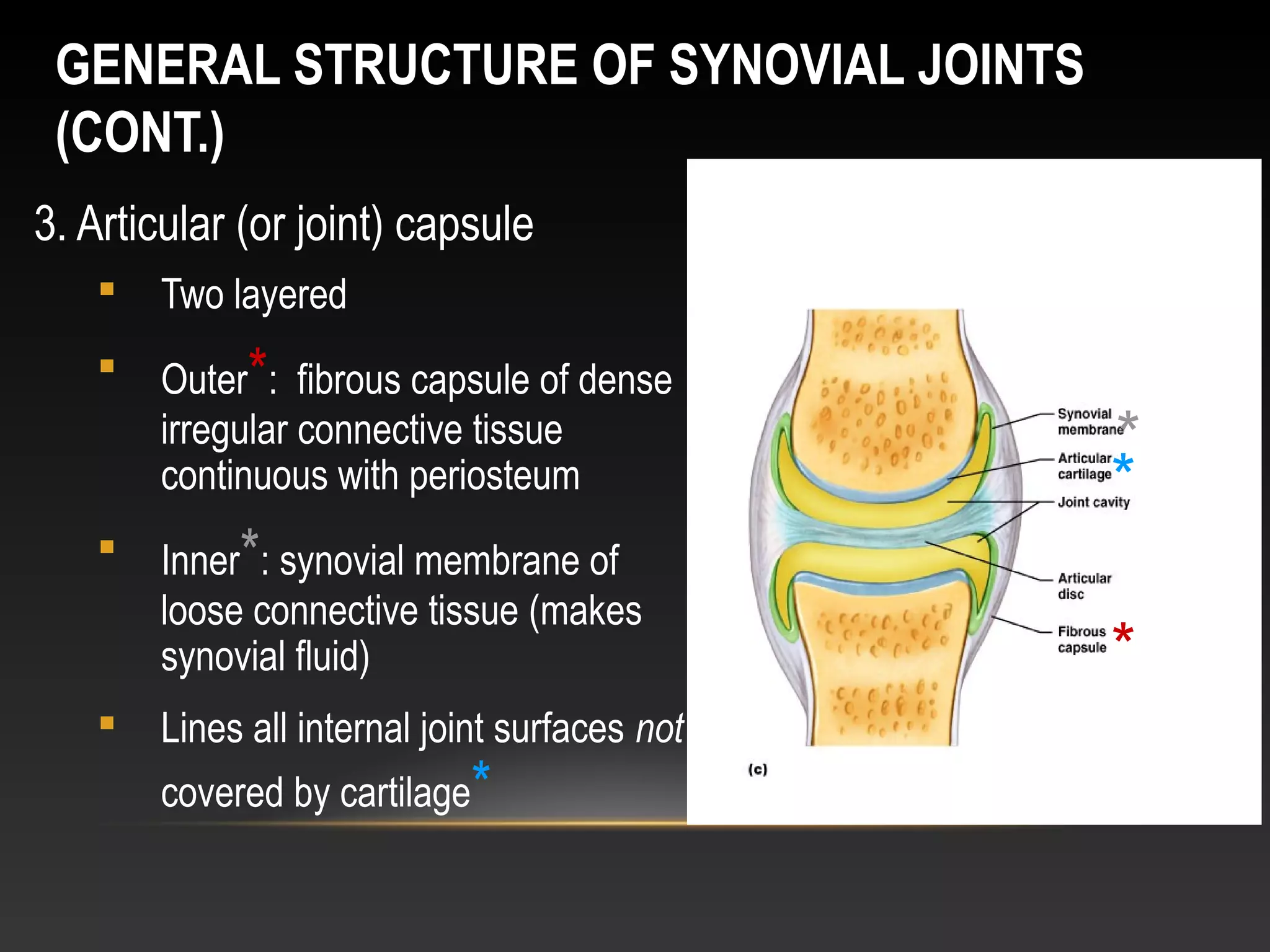











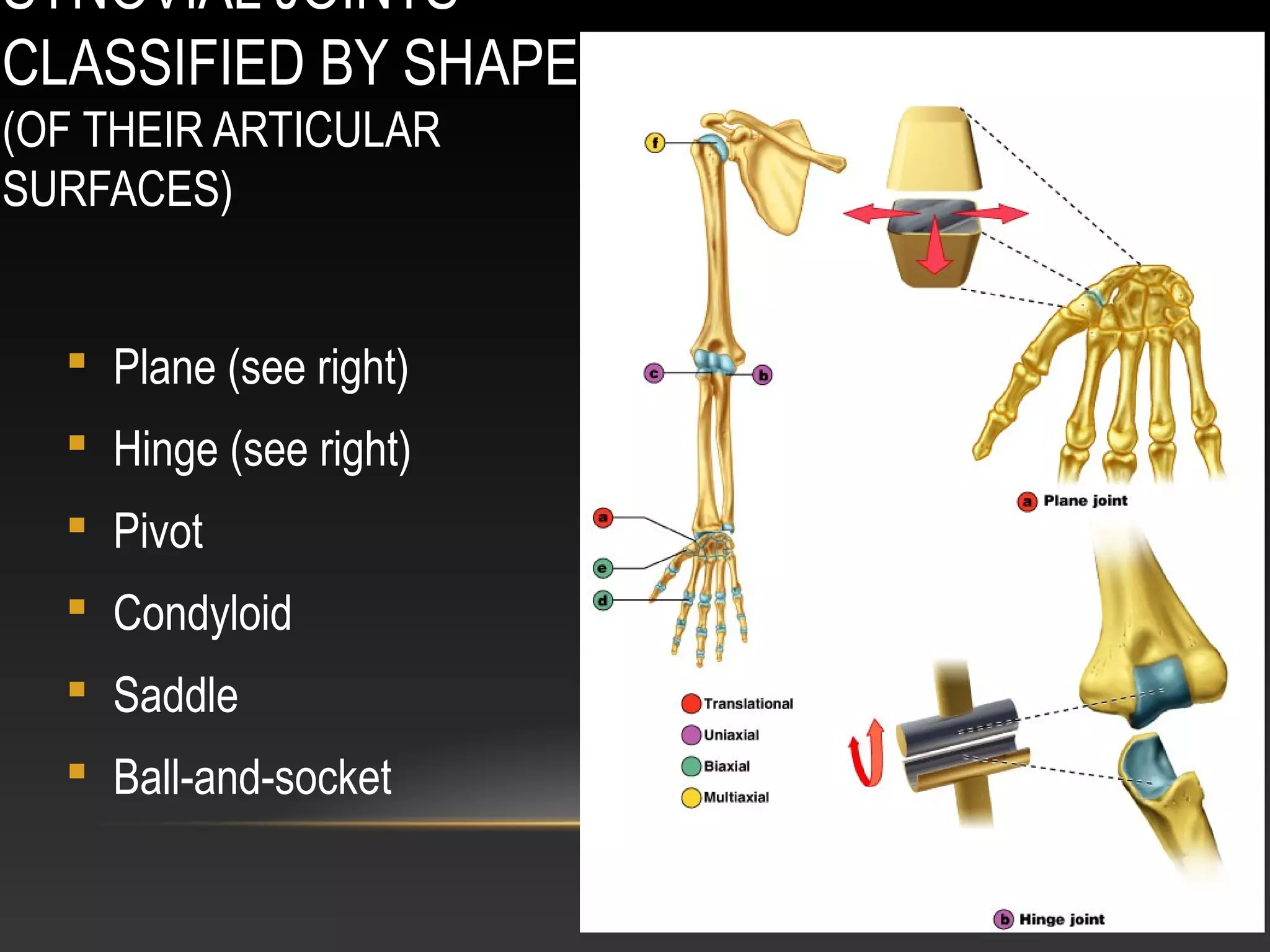














This document discusses the anatomy and classification of joints in the human body. It begins by classifying joints based on their function and structure. There are three main types of joints based on function: synarthroses (immovable), amphiarthroses (slightly movable), and diarthroses (freely movable). The document then discusses the four main structural classifications of joints: fibrous, cartilaginous, synovial, and bony. It provides examples and descriptions of different joint types within each structural classification. The majority of the document focuses on the anatomy and features of synovial joints, which are the most common and complex type of joint in the body.





































































































