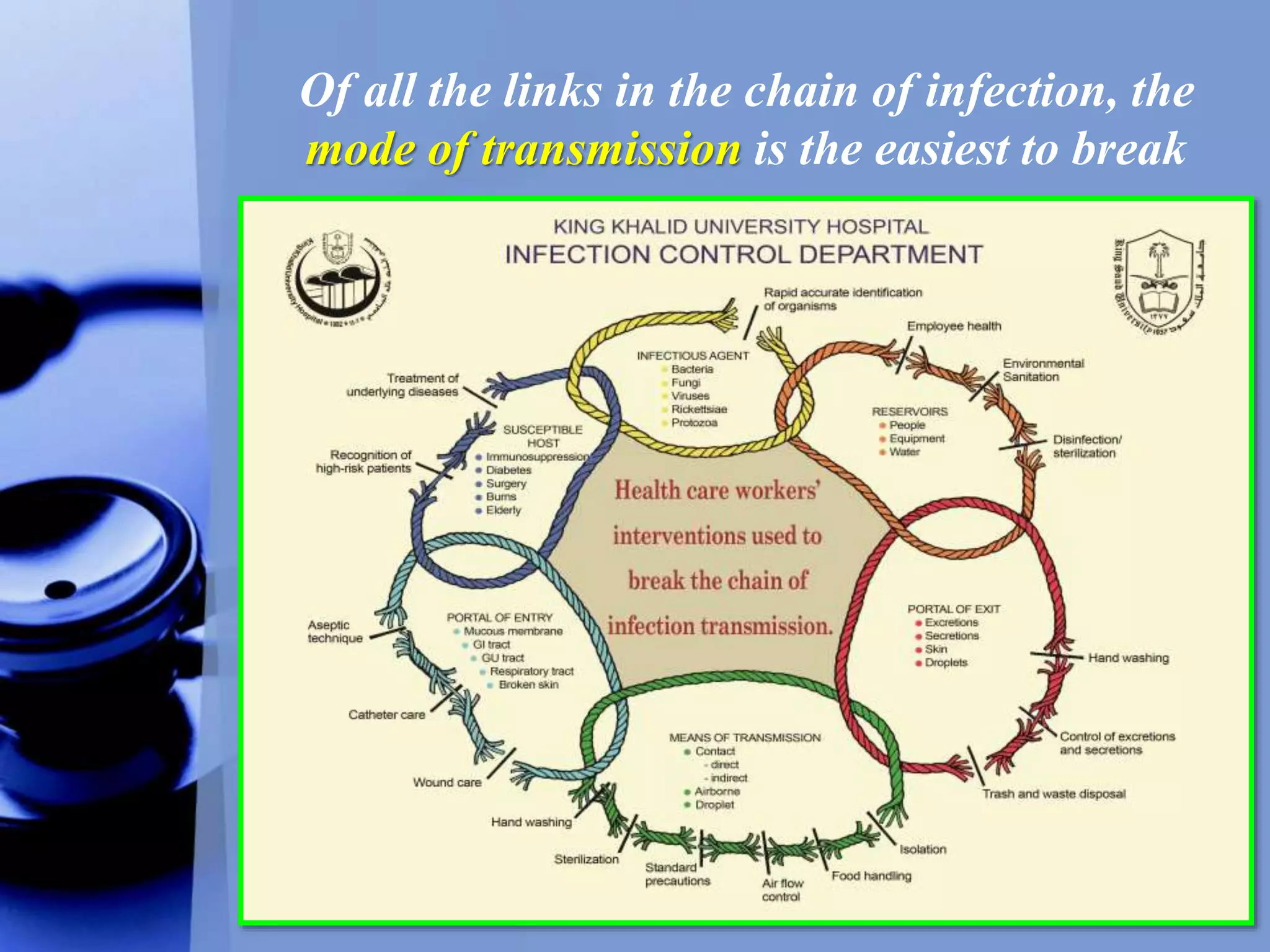
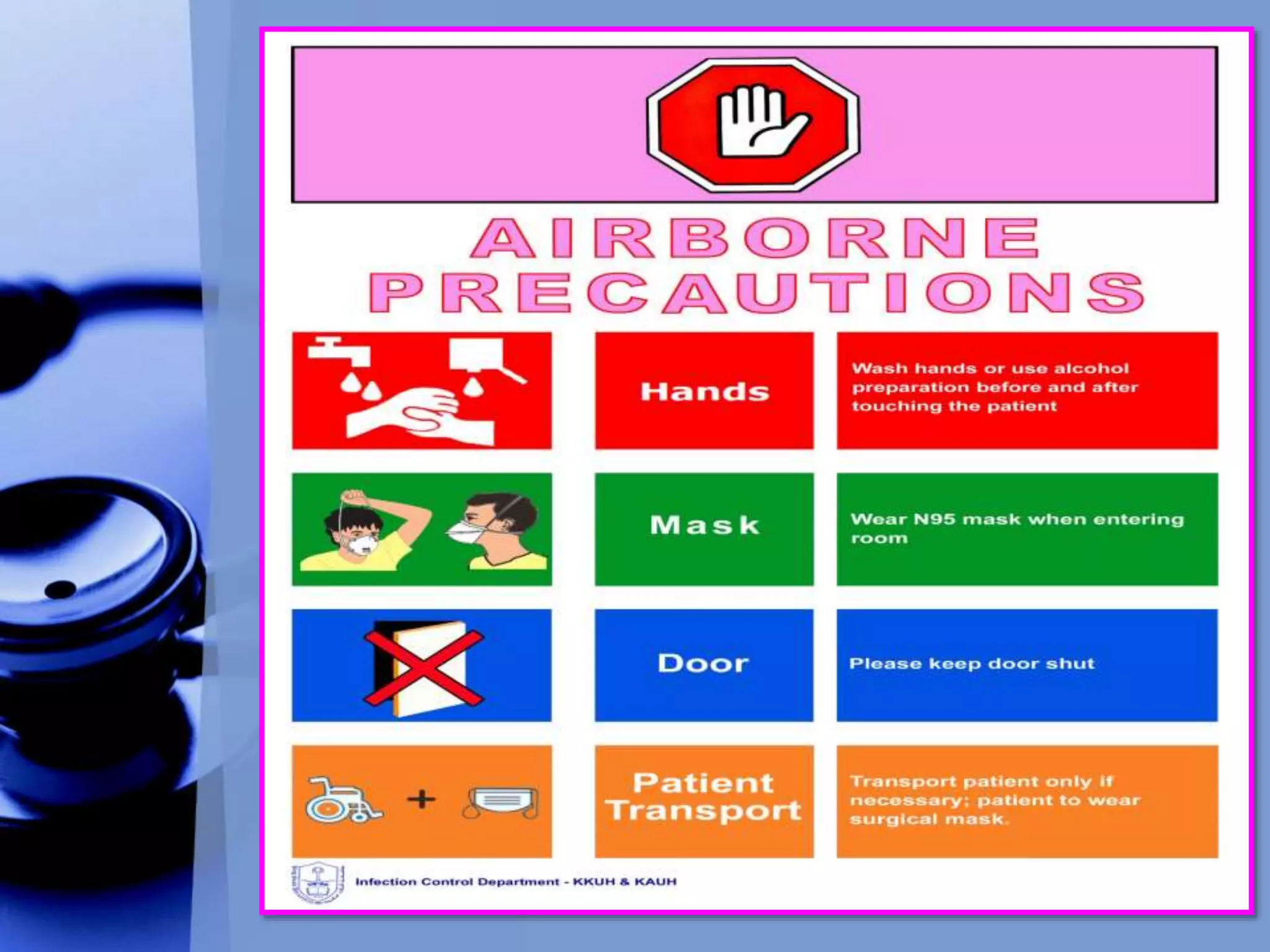
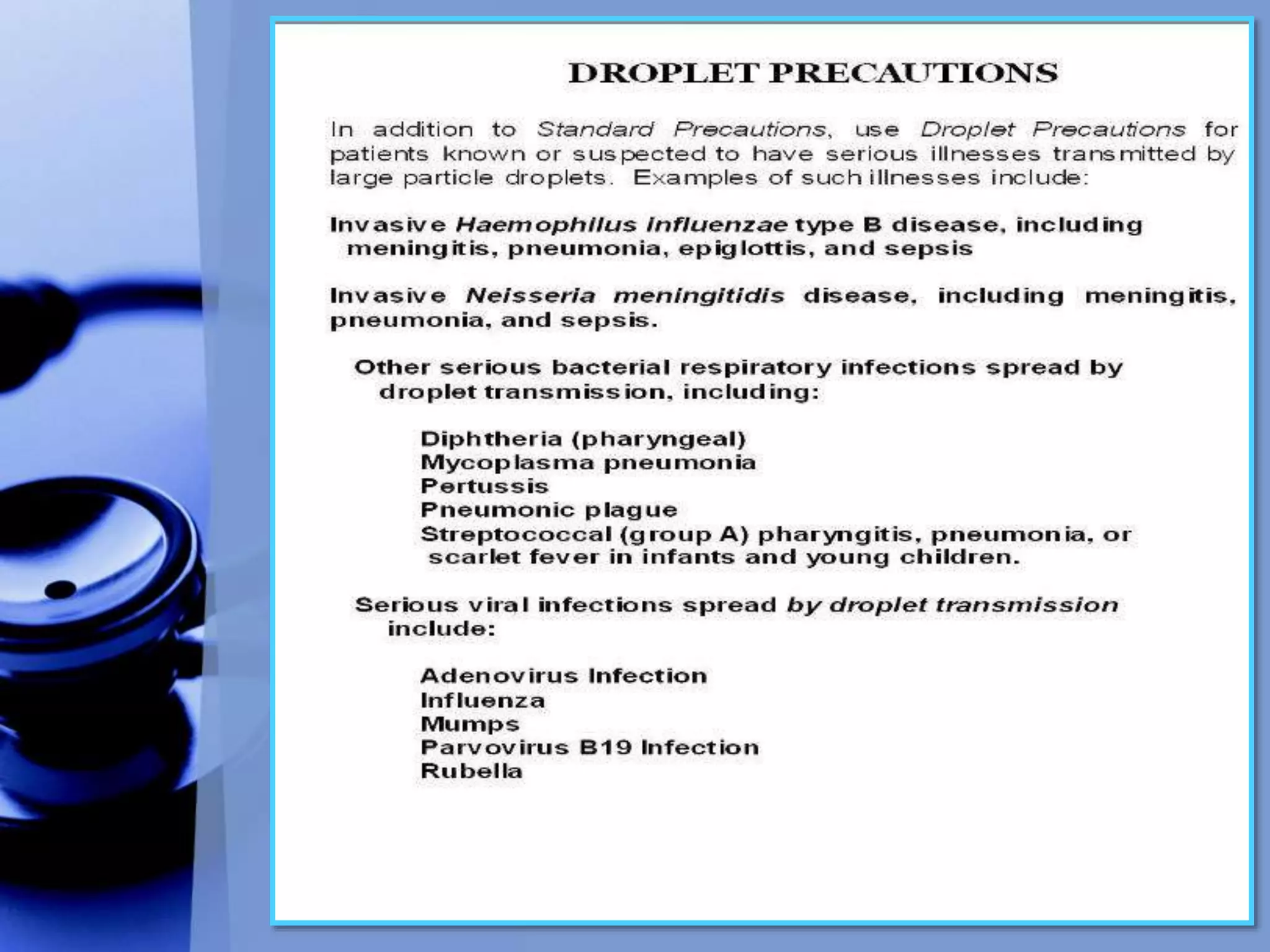
The document discusses different types of isolation precautions including airborne, droplet, and contact precautions. It provides details on causative agents, patient placement, protective equipment, and criteria for discontinuing isolation for each type of precaution. Empiric isolation is also discussed for patients presenting with certain clinical syndromes until a definitive diagnosis can be made.
























































![Infection Control Guidelines in Tuberculosis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/infectioncontrolguidlinesintuberculosiscompatibilitymode-131231005155-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































