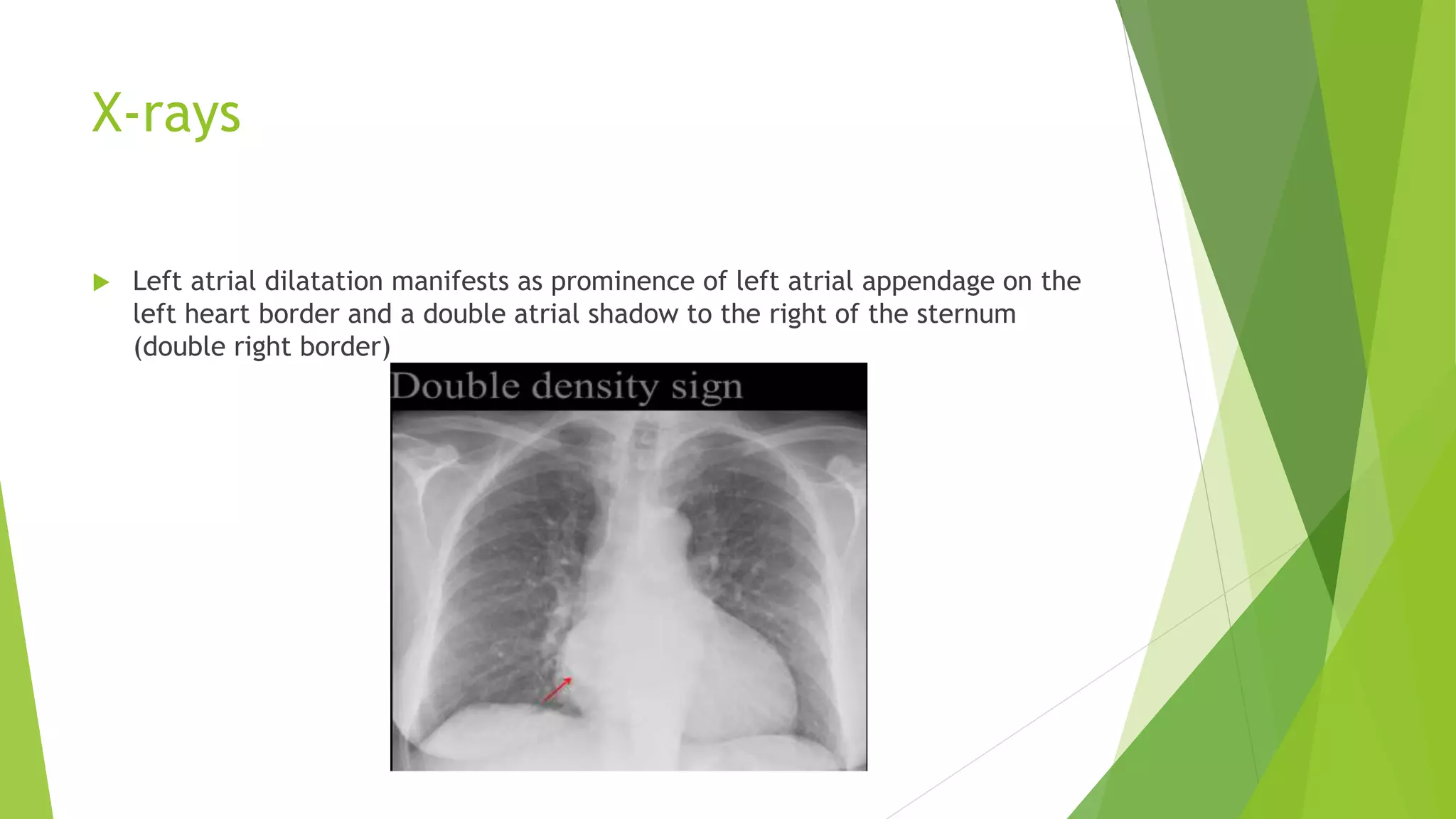
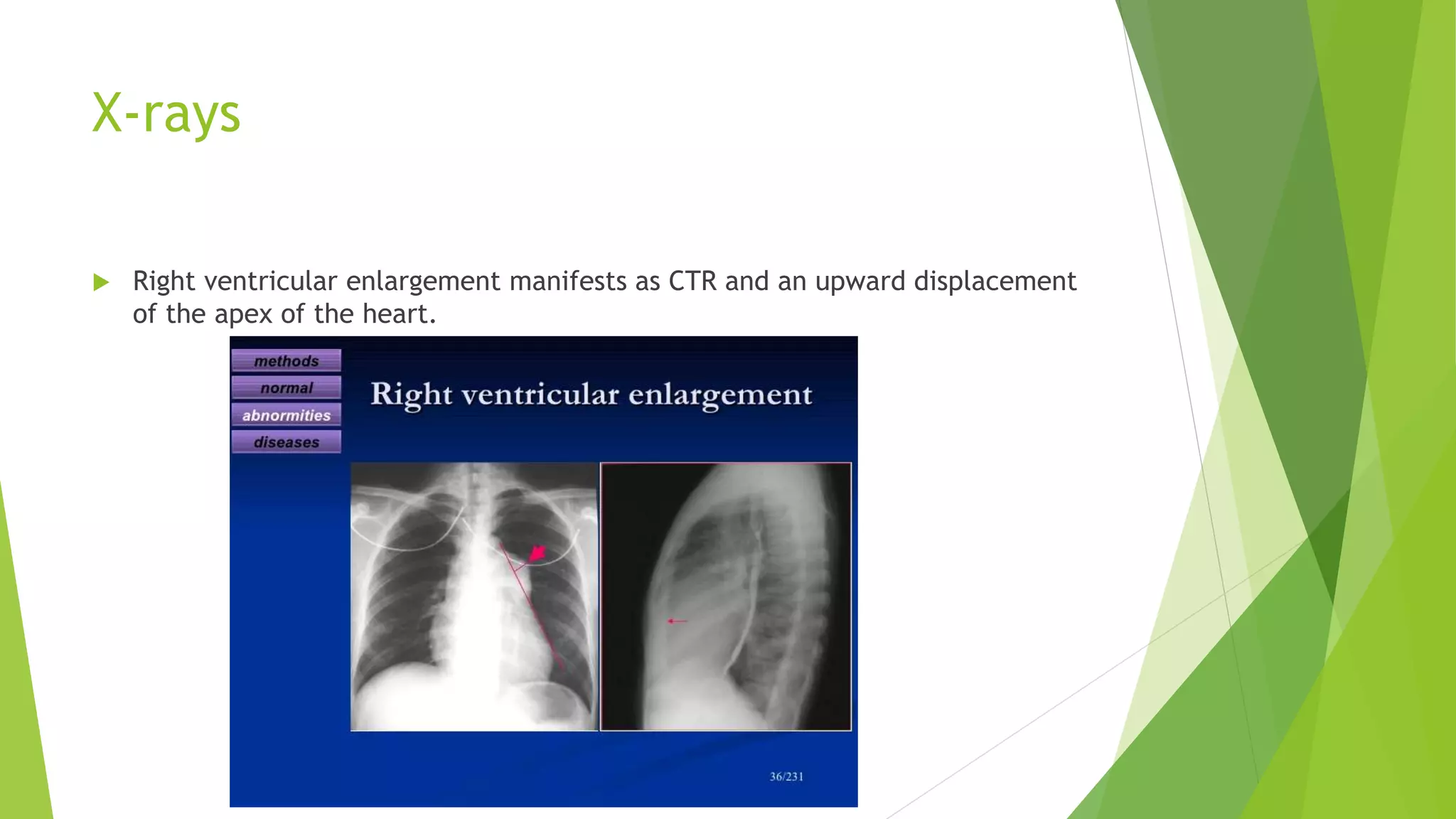
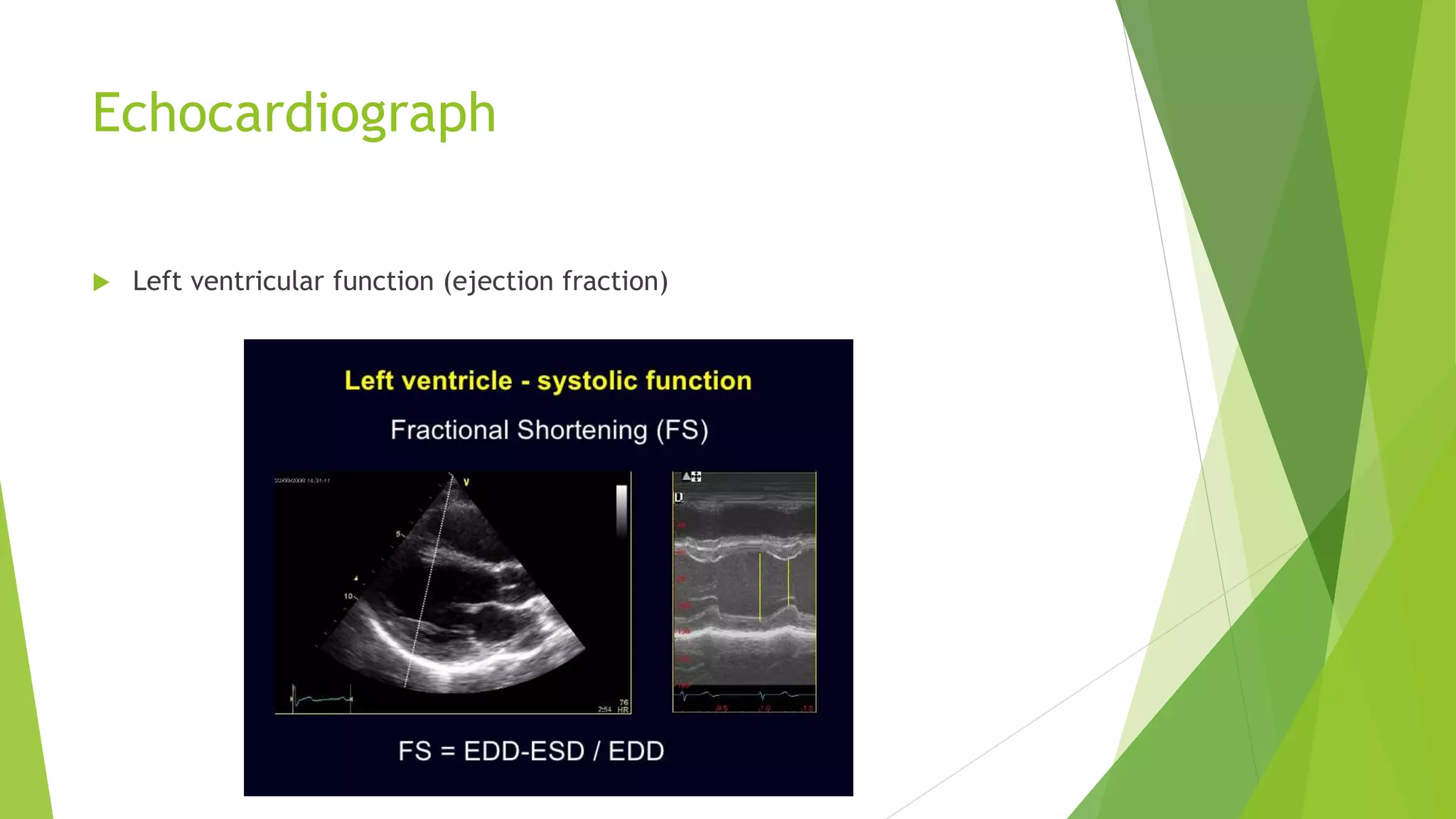
This document discusses various methods used to investigate cardiac diseases, including electrocardiography (ECG), chest x-rays, echocardiography, ambulatory ECG monitoring, radionuclide scanning, cardiac catheterization, and coronary angiography. It provides details on what each test can detect, such as arrhythmias, conduction defects, or enlarged heart chambers. Echocardiography is highlighted as a sensitive method for evaluating heart chamber size and function, including ejection fraction and wall motion. Different echocardiography techniques including 2D, M-Mode, and Doppler are described for assessing abnormalities.


















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)














