Download as PPSX, PPTX
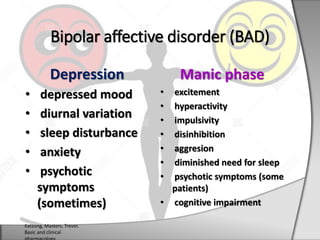

Bipolar disorder, also known as manic-depressive disorder, affects 1-3% of adults and involves alternating periods of depression and mania. During depression, patients experience symptoms like depressed mood and sleep disturbances, while manic phases involve excitement, hyperactivity, and impulsivity. The causes are unknown but may involve abnormalities in neurotransmitter systems like dopamine and norepinephrine. Bipolar disorder tends to first appear in late adolescence or early adulthood and runs in families. Lithium and anticonvulsants like valproic acid and carbamazepine are used to treat the manic phase, while antipsychotics and antidepressants are also employed.





































![Bipolar Disorder[1]](https://cdn.slidesharecdn.com/ss_thumbnails/bipolardisorder1-090518100303-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

