Downloaded 186 times


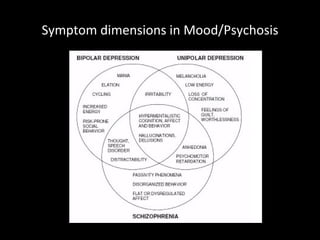
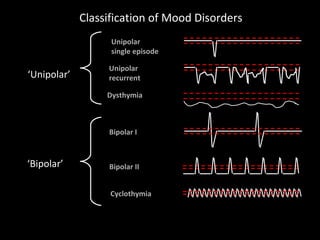
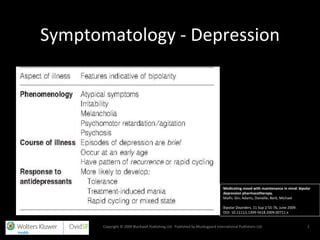



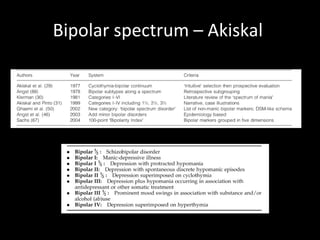
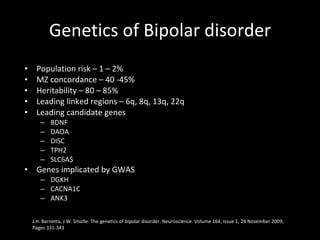






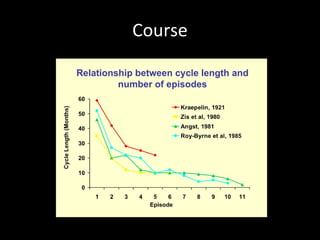
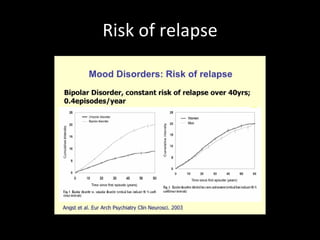













The document provides an overview of bipolar disorder, including its prevalence, symptoms, diagnosis, course, treatment guidelines, and monitoring recommendations. It discusses the symptomatology and classification of bipolar I and II disorders. It also outlines the etiology, neurobiology, and risk of relapse associated with bipolar disorder. Treatment guidelines from NICE focus on acute stabilization and long-term management using lithium, anticonvulsants, or antipsychotics.



































![Bipolar Disorder[1]](https://cdn.slidesharecdn.com/ss_thumbnails/bipolardisorder1-090518100303-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















































