Downloaded 25 times

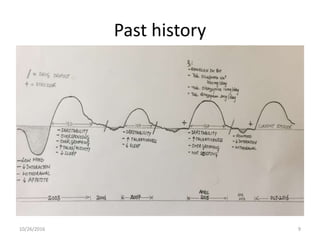
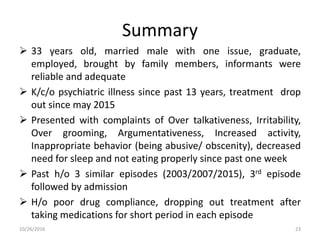
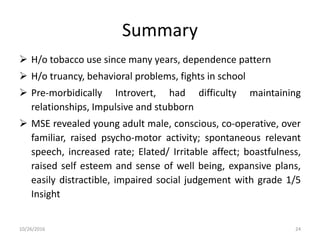


A 33-year-old male with an extensive history of psychiatric illness presented with symptoms of over talkativeness, irritability, and inappropriate behavior following a job promotion, leading to hospitalization. Diagnosed with bipolar affective disorder, he received a combination of medications including neuroleptics and mood stabilizers, alongside psychoeducation for his family. The treatment plan emphasized regular follow-up and monitoring to ensure medication adherence and proper management of his condition.



















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









