Download to read offline
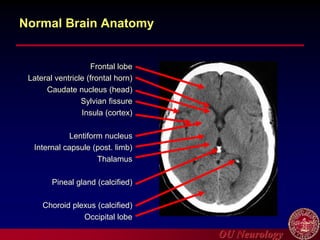
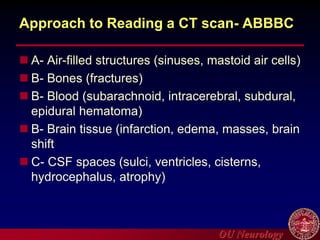
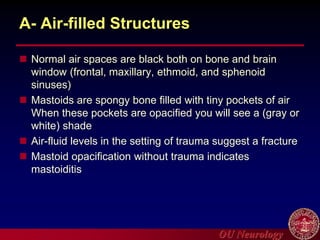
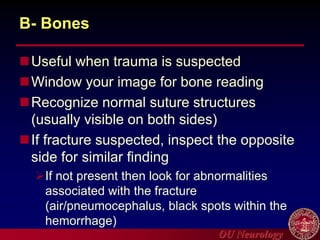
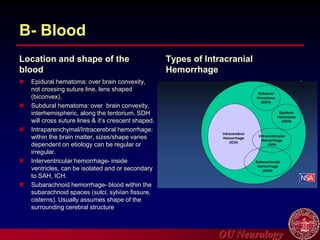
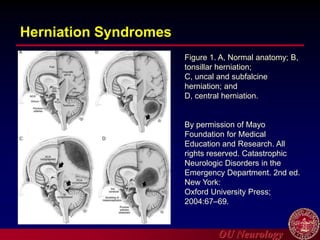
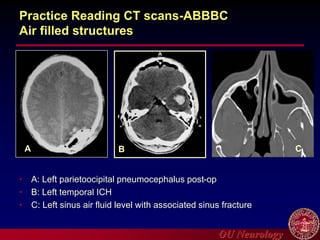

This document provides an introduction to head CT imaging. It discusses the basics of CT, including how it uses x-rays to provide axial brain views and measures tissue density. It outlines an ABBBC approach to reading CT scans, focusing on air-filled structures, bones, blood, brain tissue, and CSF spaces. The document reviews normal brain anatomy and identifies various pathologies that can be seen on head CT such as hemorrhages, infarcts, masses and herniations. It provides examples of interpreting CT scans using the ABBBC method.























![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)




















































