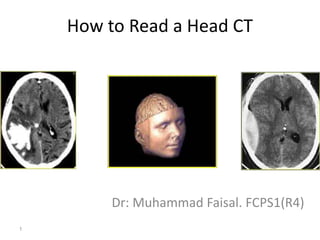
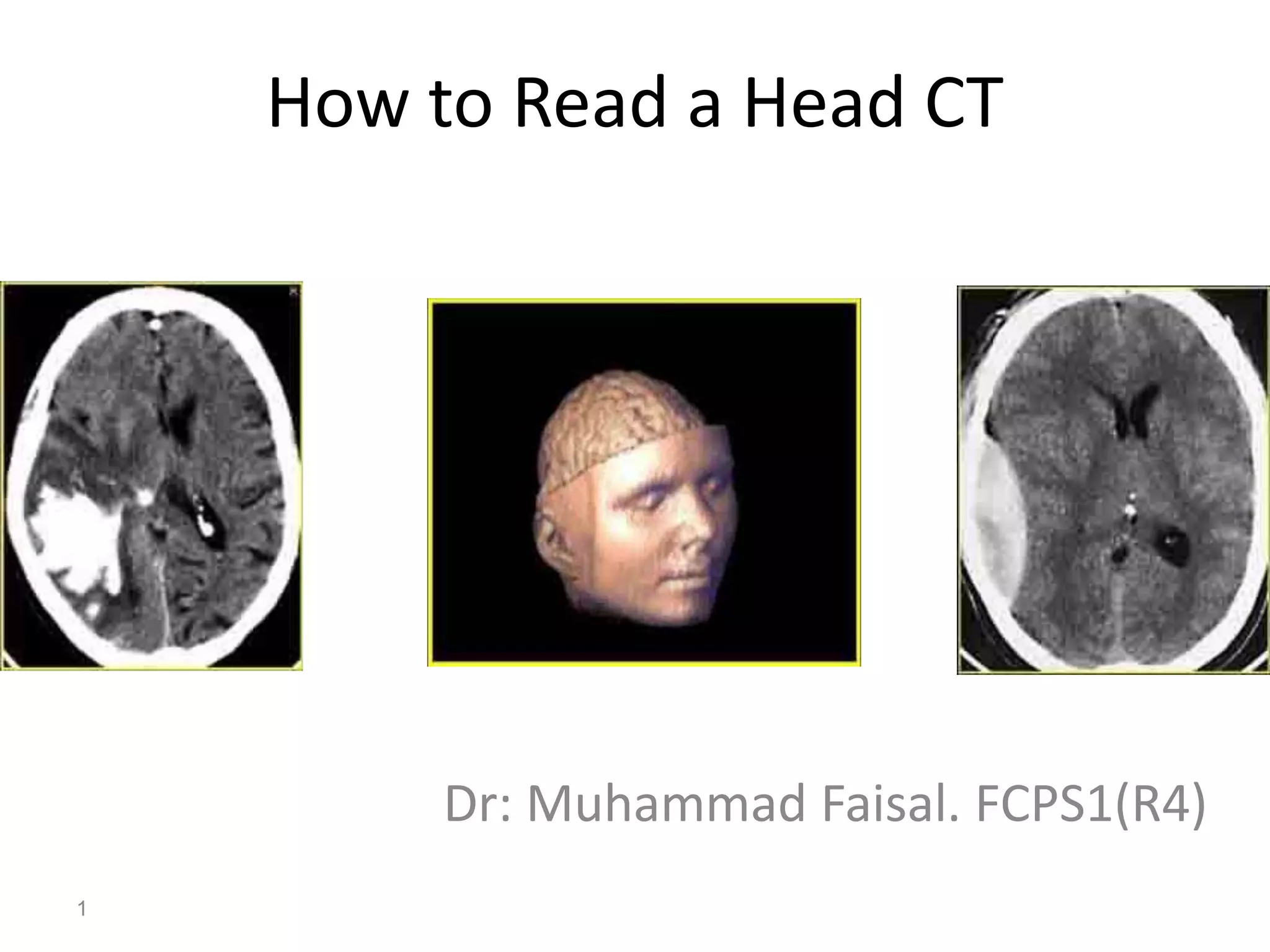
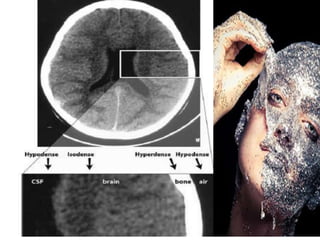
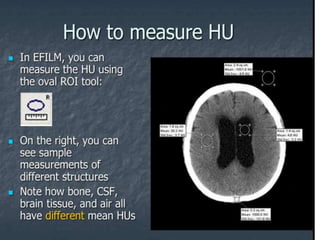
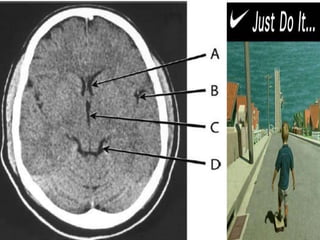
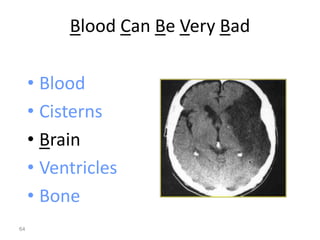
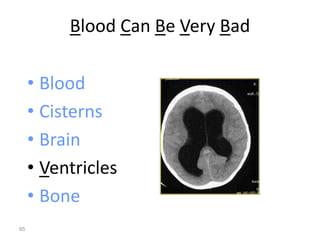
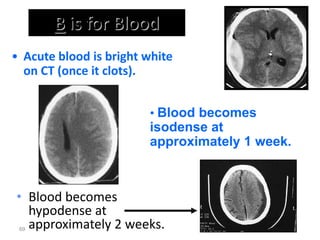
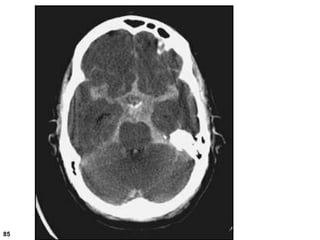
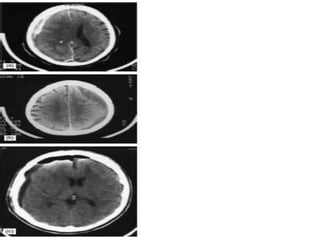
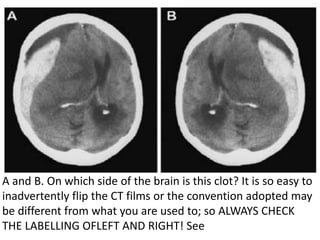
The clot is on the right side of the brain. The labeling at the top of the image indicates "R" for right. It's important to always verify the left/right labeling when interpreting images to avoid potential mistakes from flipped or differently labeled images.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














