This document summarizes intestinal obstruction, including:
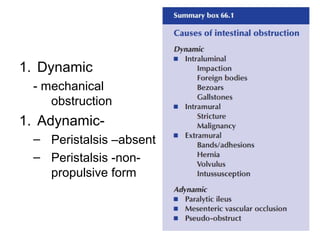
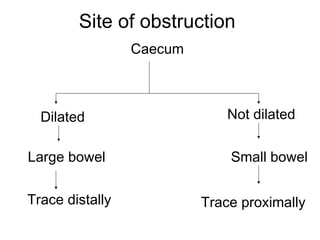
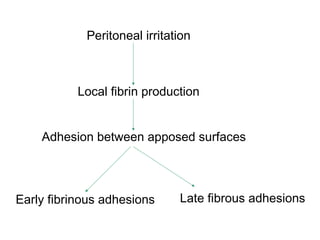
1. The pathology and clinical features of mechanical obstruction proximal and distal to the obstruction site. Distension results from gas, fluid, and electrolyte imbalances.
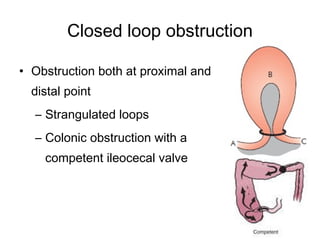
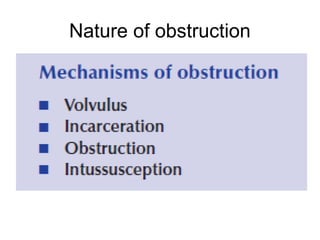
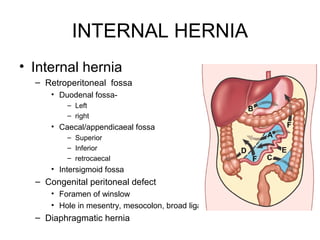
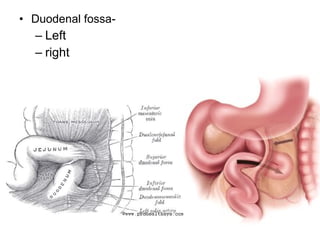
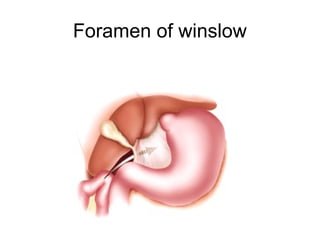
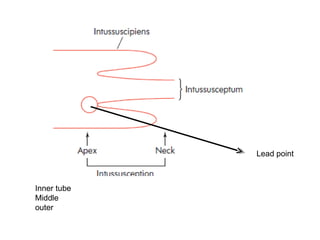
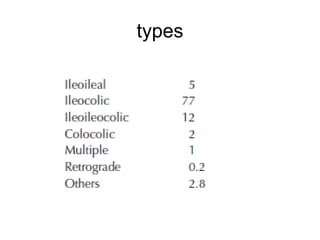
2. Types of obstruction include internal and external strangulation, closed loop, and special types like internal hernia, strictures, and intussusception.
3. Clinical features include the classic pain, vomiting, distension, and constipation quartet. Treatment involves gastrointestinal drainage, fluid replacement, and surgical relief of the obstruction.