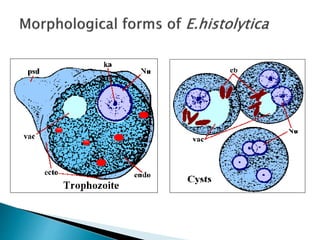
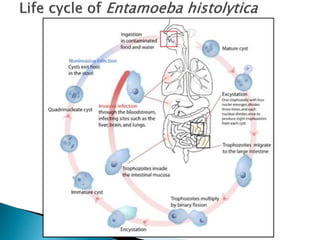
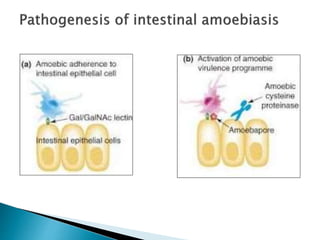
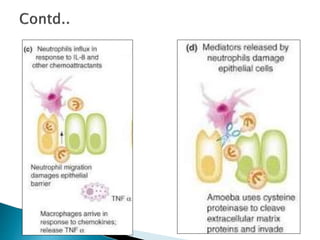
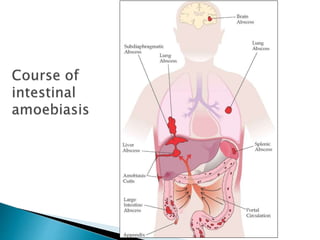
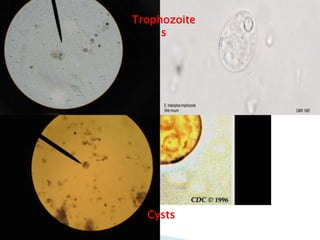
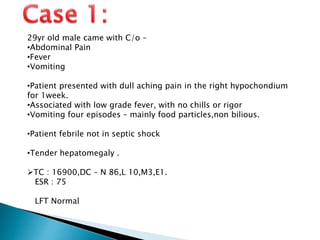
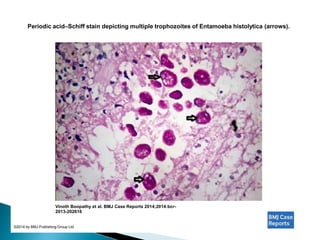
Amebiasis is caused by the protozoan Entamoeba histolytica. It commonly involves the intestines but can spread to other organs. Symptoms range from mild diarrhea to severe colitis or liver abscesses. Diagnosis involves identifying the trophozoites or cysts in stool or abscess samples. Treatment includes metronidazole combined with luminal amebicides like diloxanide furoate.