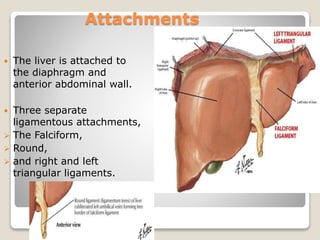
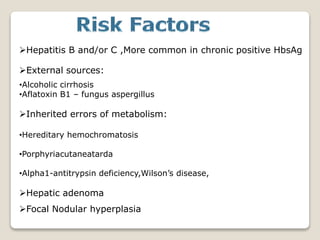
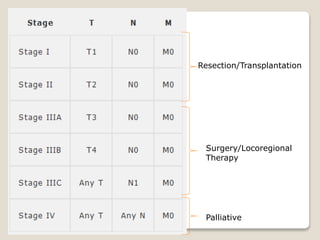
HCC is a primary malignancy of the liver that is usually preceded by cirrhosis. Risk factors include hepatitis B and C infection, alcohol use, and aflatoxin exposure. Presentation may be asymptomatic initially, but can include abdominal pain, weight loss, and jaundice. Diagnosis involves blood tests like AFP and liver imaging with ultrasound, CT, or MRI. Treatment depends on tumor stage and liver function, and may include surgery, ablation, embolization, targeted therapy, or palliation. Prevention strategies focus on hepatitis B vaccination, screening high risk groups, and treating chronic liver disease early.



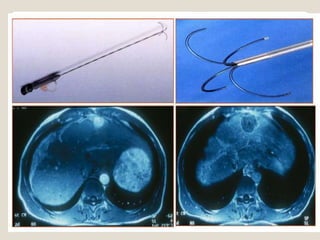
![Local Regional Therapy
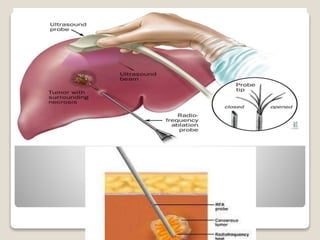
Ablation: inducing direct necrosis
Chemical : ethanol (PEI), acetic acid
Physical: radiofrequency ablation [RFA], microwave ablation,
Cryoablation
Laparoscopic, percutaneousor open approaches.
Indications: local disease only completely amenable to
ablative therapy according to the size and location of the
tumor(s).
Tumor necrosis is assessed by CT/MRI at intervals an no
contrast uptake](https://image.slidesharecdn.com/73hgfxjsesbawsdijoag-signature-6a4fba10d9d2b0f1e4c2c34cd672cb8ae62d8e409b4892251c485a275b1c449b-poli-180920055637/85/Hcc-32-320.jpg)