Download to read offline

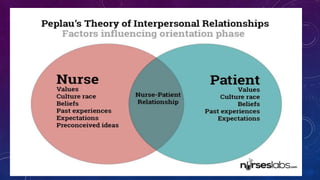



This document discusses Hildegard Peplau's theory of interpersonal relations in nursing. It outlines Peplau's concepts of person, environment, and health. It also describes the six nursing roles in Peplau's theory - stranger, resource, teacher, counselor, surrogate, and leader. Finally, it summarizes Peplau's four developmental stages of the nurse-client relationship: orientation, identification, working, and resolution/termination.