Download as PDF, PPTX





The document presents insights from Lorraine D. Ellis and William Gluck on integrating clinical operations and clinical data management using electronic data capture (EDC). It discusses the evolution from traditional monitoring processes to real-time monitoring, emphasizing the importance of integration between clinical operations and data management for improved efficiency. The speakers advocate for leveraging technology to enhance data quality, streamline processes, and foster continuous communication in clinical trials.
Introduces Lorraine D. Ellis and William Gluck, their roles, and backgrounds in clinical research.
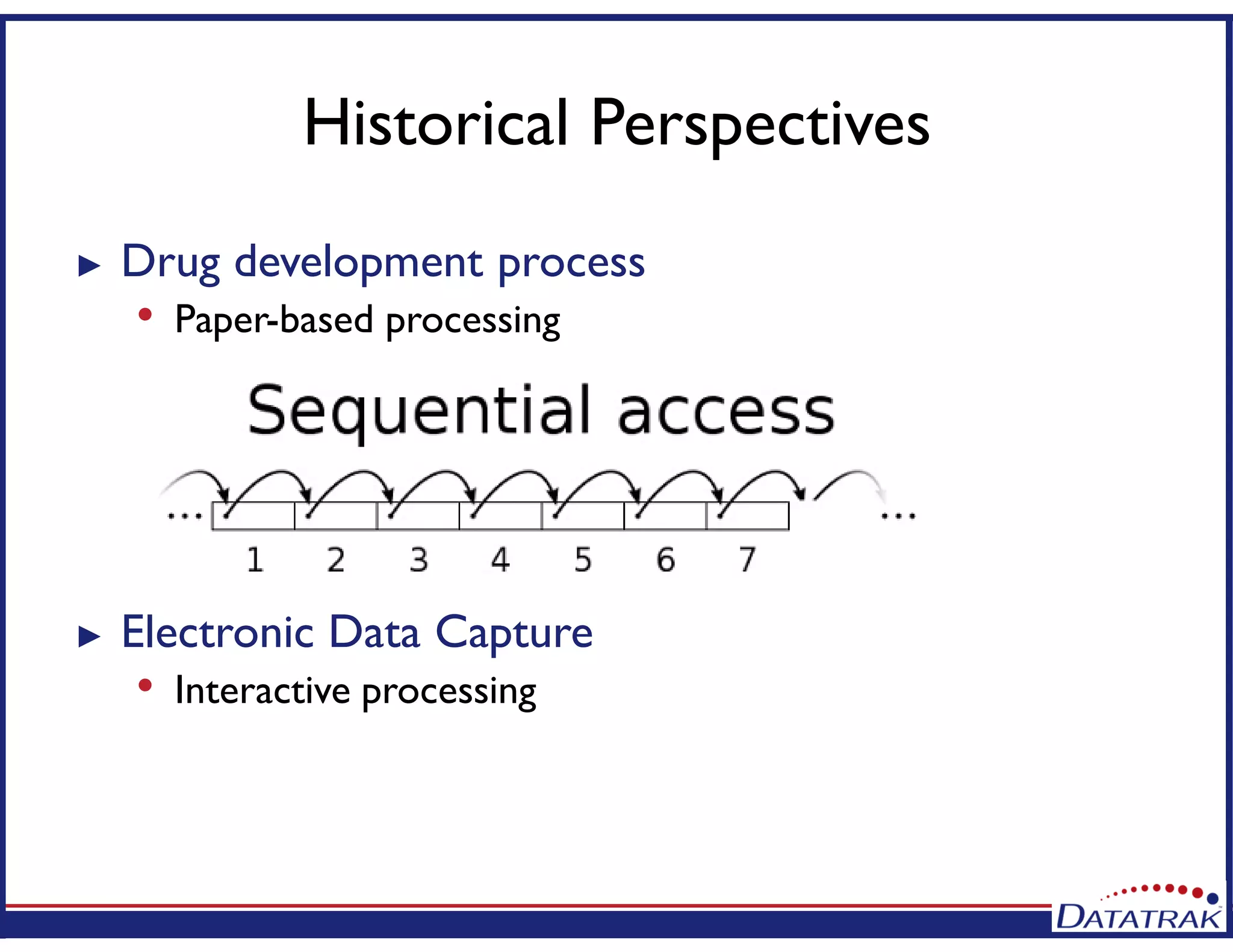
Discusses how technology has advanced in clinical operations, especially in monitoring and data management.
Highlights EDC benefits including real-time monitoring, improved data quality, and enhanced feedback.
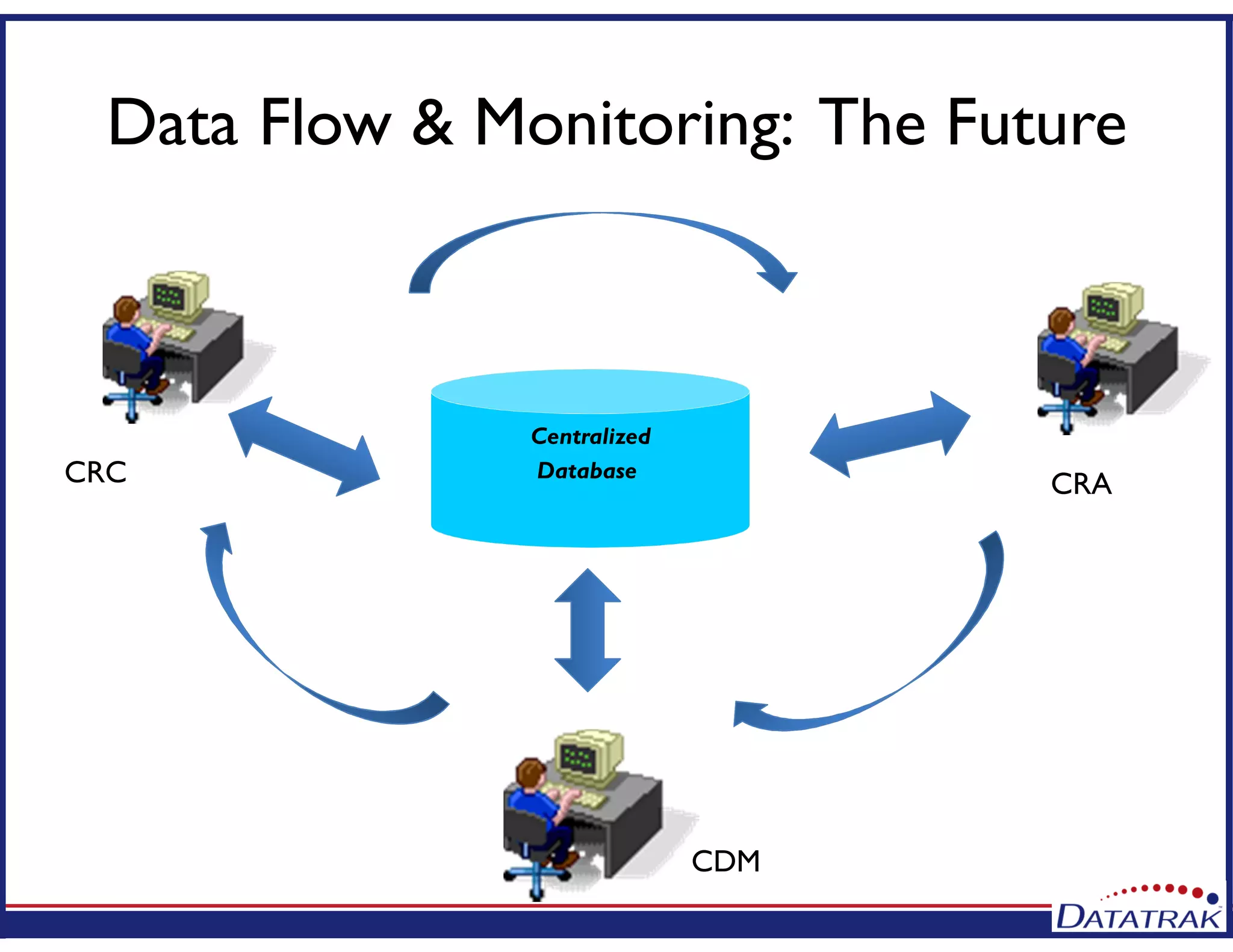
Explores the future of clinical operations emphasizing real-time data flow and reduced silos in processes.
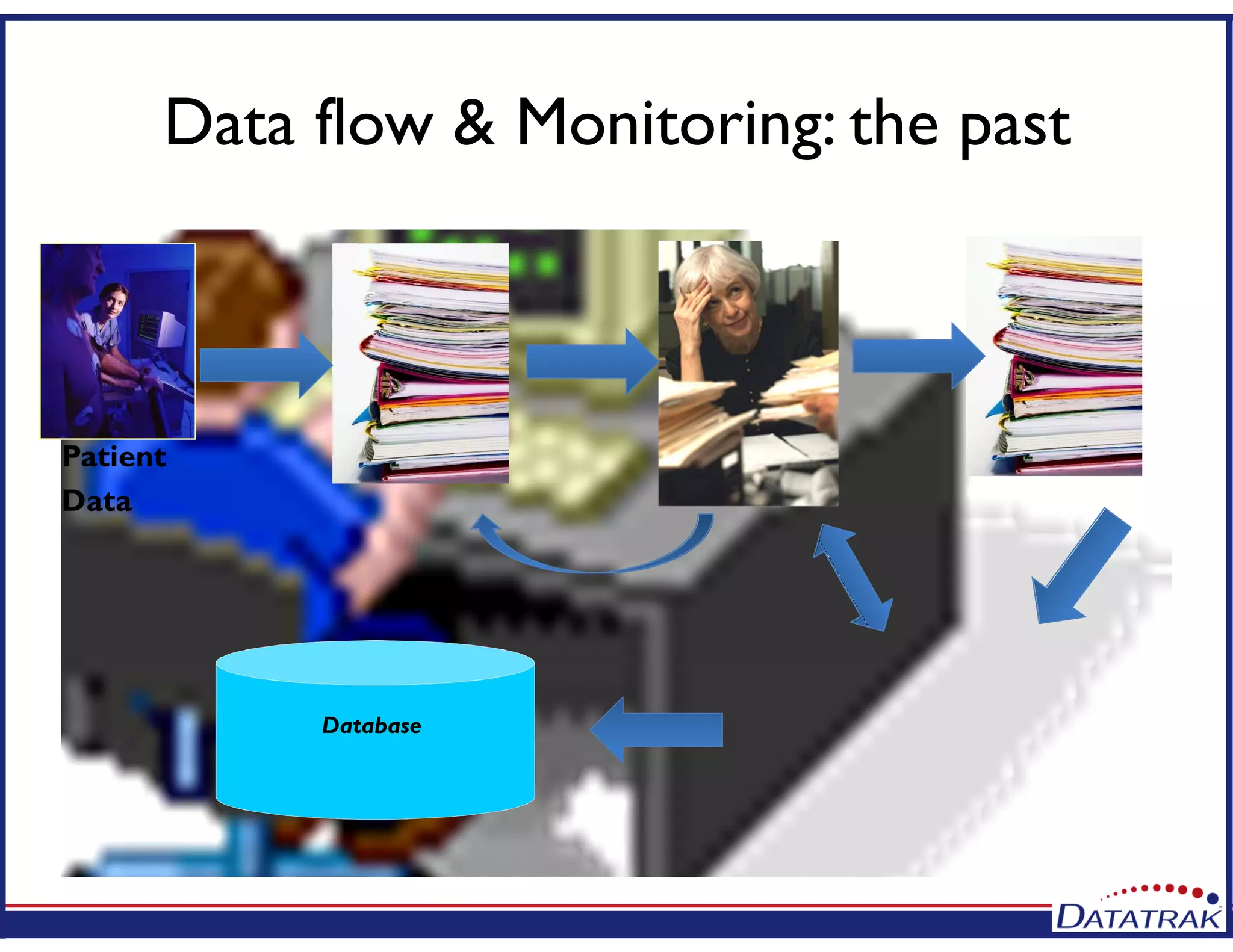
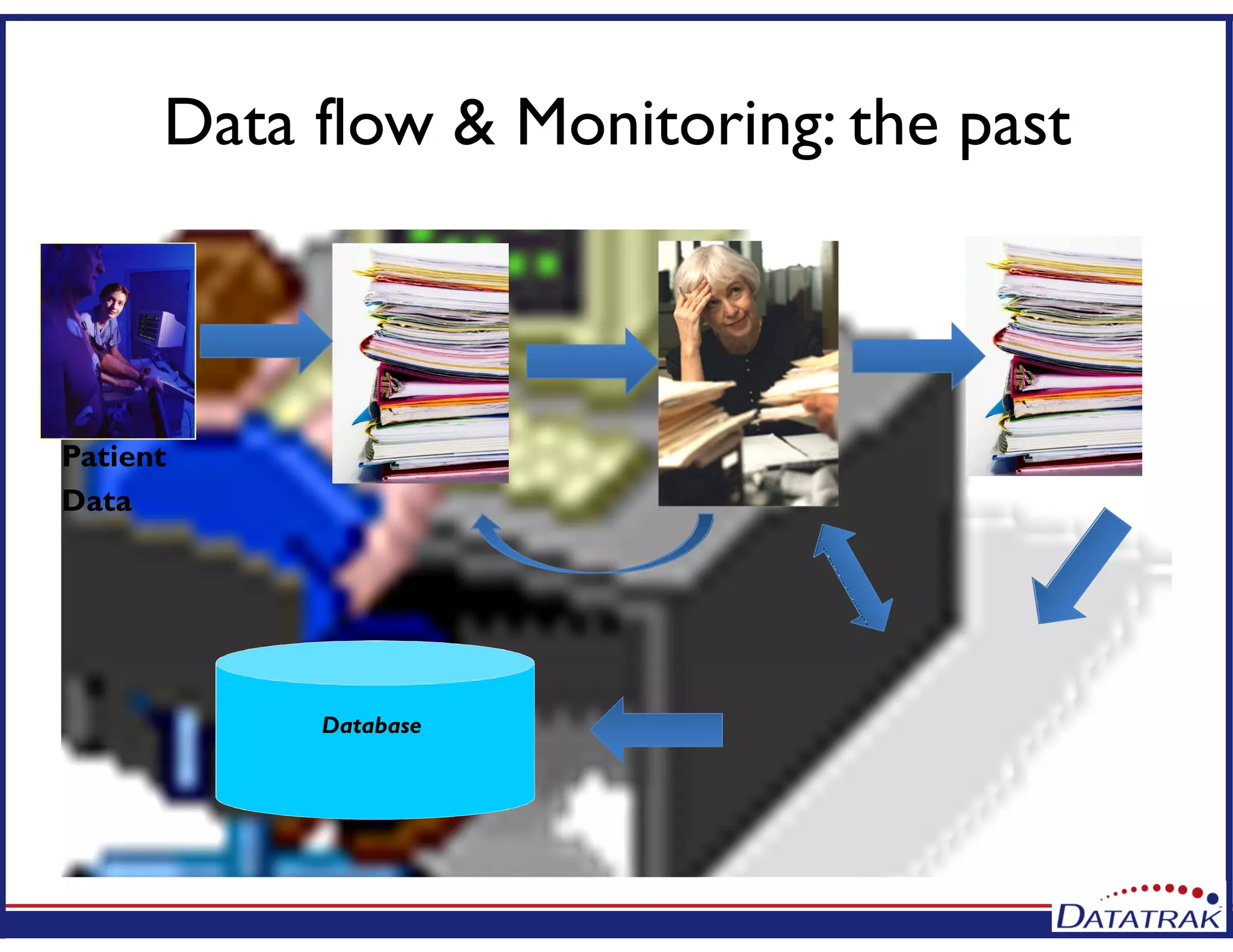
Comparison of data flow and monitoring processes from the past to future centralized processes.
Outlines agenda, highlights process-driven approaches, and emphasizes integration in clinical data management.
Shares case studies illustrating the challenges and successes in EDC implementation in clinical settings.
Concludes on the need for integrating technology into re-engineered processes for improved outcomes.
Provides contact information for the speakers and opens the floor for questions.