
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Inguinal canal final
Similar to Inguinal canal final (20)
Recently uploaded
Recently uploaded (20)
Inguinal canal final
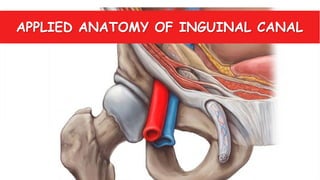
- 1. APPLIED ANATOMY OF INGUINAL CANAL
- 2. EXTERNAL OBLIQUE INTERNAL OBLIQUE TRANSVERSUS ABDOMINIS FASCIA TRANSVERSALIS INGUINAL LIGAMENT EXTERNAL OBLIQUE APONEUROSIS BLADDER RECTUS ABDOMINIS CREMASTERIC MUSCLE
- 3. WHAT IS INGUINAL CANAL?? • Oblique fibromuscular passage in the lower part of anterior abdominal wall, situated just above the medial half of inguinal ligament. • LENGTH & WIDTH: 4 cm long & 1 cm broad • DIRECTION: Downwards, Forwards & Medially
- 5. EXTENSION: Deep inguinal ring to Superficial Inguinal ring DEEP INGUINAL RING : • Beginning of Inguinal Canal. • Oval opening in fascia transversalis. • Lies 1.25cm above midinguinal point. • From its margins, the fascia transversalis is prolonged to form one of the covering called the internal spermatic fascia of the spermatic cord. DEEP INGUINAL RING SUPERFICIAL INGUINAL RING SUPERFICIAL INGUINAL RING : • End of Inguinal Canal. • Triangular defect in external oblique aponeurosis. • Apex points superolaterally and base is formed by pubic crest • Two remainining sides of triangle are called medial crus and lateral crus, and are attached to pubic symphysis and pubic tubercle respectively. • At the apex of triangle, two crura are held together by crossing intercrural fibres which prevent further widening of superficial inguinal ring. • From its margins, the external oblique aponeurosis is prolonged to form another covering called the external spermatic fascia of the spermatic cord.
- 6. BOUNDARIES OF INGUINAL CANAL ANTERIOR WALL & FLOOR: EXTERNAL OBLIQUE APONEUROSIS INTERNAL OBLIQUE INGUINAL LIGAMENT
- 7. ROOF: TA Arching fibres of internal oblique Arching fibres of transversus abdominis Conjoint tendon Arching fibres of transversus abdominis Arching fibres of internal oblique
- 8. POSTERIOR WALL : Conjoint tendon CONJOINT TENDON FASCIA TRANSVERSALIS
- 9. CONTENTS OF INGUINAL CANAL Ductus deferens & its artery Testicular vessels & pampiniform plexus Cremasteric vessels Internal spermatic fascia Cremasteric muscle External spermatic fascia Genital branch of genitofemoral nerve Remains of processus vaginalis Ilioinguinal nerve
- 10. HESSELBACH’S TRIANGLE Medial umbilical ligament
- 11. CLINICAL ANATOMY
- 12. CREMASTERIC REFLEX Touch on anterior aspect of superomedial part of thigh Ilioinguinal nerve carries sensation to the spinal cord at level L1 Simulation of motor fibres of genital branch of genitofemoral n. Contraction of cremateric muscle and elevation of testis • Cremasteric reflex in children : Hyperactive • May be helpful to diagnose upper and lower motor lesions and/or spinal injury at L1-L2 level
- 13. DEFENCE MECHANISMS OF INGUINAL CANAL • FLAP-VALVE MECHANISM: Inguinal Canal – Site of potential weakness in lower anterior abdominal wall & may provide site for herniation. WALLS ARE APPROXIMATED
- 14. • SLIT-VALVE MECHANISM : LATERAL & MEDIAL CRUS APPROXIMATED BALL- VALVE MECHANISM : UPWARD PULLING OF TESTES BY CREMASTERIC MUSCLE
- 15. SHUTTER MECHANISM : GUARDING MECHANISM: Deep inguinal ring – guarded anteriorly by Internal oblique Superficial inguinal ring – guarded posteriorly by Conjoint tendon & reflected part of inguinal ligament. Contraction of Internal Oblique and Transversus abdominis
- 16. INGUINAL HERNIA
- 17. WHAT IS HERNIA? • Hernia is a condition in which part of an organ is displaced & protrudes through the wall of the cavity containing it. • Hernia : 1) Sac 2)Coverings of the sac 3) Contents of sac
- 18. INGUINAL HERNIA • An inguinal hernia is the protrusion or passage of peritoneal sac, with/without abdominal contents through a weakened part of abdominal wall in the groin. • Cause: peritoneal sac enters the inguinal canal either through deep inguinal ring or through posterior wall of inguinal canal. • Inguinal hernia are therefore, mainly classified as DIRECT & INDIRECT.
- 19. INDIRECT INGUINAL HERNIA • Most common of the two types. • Occurs because some part or all, of the embryonic processus vaginalis remains open or patent & hence, it is referred to as congenital indirect inguinal hernia. • The protruding peritoneal sac enters the inguinal canal by passing through deep inguinal ring. • Protrusion occurs lateral to the inferior epigastric vessels. • The extent of protrusion down the inguinal canal depends on the amount of processus vaginalis that remains patent.
- 20. According to extent of indirect inguinal hernia , they are of two main types: INCOMPLETE : • Bubonocele: Here, sac is confined to inguinal canal • Funicular: Here, sac crosses the superficial ring but doesn’t reach the bottom of the scrotum. COMPLETE : • Here, sac descends to the bottom of the scrotum. COVERINGS: Same as Spermatic cord Bubonocele Funicular Complete
- 21. DIRECT INGUINAL HERNIA • Peritoneal sac enters the medial end of inguinal canal directly through weakened posterior inguinal wall. • It is usually acquired. • Protrusion occurs medial to inferior epigastric vessels i.e. in Hesselbach’s triangle.
- 22. COVERINGS: MEDIAL DIRECT INGUINAL HERNIA LATERAL DIRECT INGUINAL HERNIA Extra peritoneal tissue Extra peritoneal tissue Fascia transversalis Fascia transversalis Conjoint tendon Cremasteric fascia External Spermatic fascia External Spermatic fascia Skin Skin
- 23. DIFFERENCE BETWEEN DIRECT & INDIRECT INGUINAL HERNIA CHARACTERISTIC DIRECT INGUINAL HERNIA INDIRECT INGUINAL HERNIA Acquired/Congenital Acquired Acquired or Congenital Site of protrusion Posterior wall of canal Deep inguinal ring Extent Rarely scrotum Generally scrotum Neck Lies medial to inferior epigastric vessels Lateral to inferior epigastric vessels Age group Middle and old age Can be in Young age Internal ring occlusion test Negative Positive
- 24. PENTALOON HERNIA (DOUBLE, ROMBERG, SADDLE) • Both direct and indirect inguinal sac re present and clinically present as direct hernia. • During surgery, indirect sac may remain unrecognized and so, leads to recurrent hernia. • Medial and Lateral sacs protrudes on either side of inferior epigastric vessels.
- 25. SLIDING INGUINAL HERNIA • Posterior wall of sac is not only formed by parietal peritoneum but also by sigmoid colon with its mesentery on left side; cecum on right side and often with a portion of bladder.
- 26. STRANGULATED HERNIA • A Strangulated hernia is a hernia that cuts off the blood supply to intestines and tissues in the abdomen. • Leads to formation of gangrene. CAUSES: 1)Narrow neck 2)Adhesions 3)Irreducibility
- 27. DIAGNOSIS INTERNAL RING OCCLUSION TEST • Procedure: After reducing the herniated contents and occluding the deep inguinal ring, patient is asked to cough. • Observation: 1) Swelling occur medial to thumb Direct inguinal hernia 2) Swelling absent and appear after releasing the thumb Indirect inguinal hernia
- 28. THREE FINGER TEST (ZIEMEN TEST) Indirect Inguinal hernia
- 29. TREATMENT It includes:- • Open Repair a)Lichtenstein(Tension free) repair (HERNIOPLASTY) b)McVay (Cooper’s Ligament) repair: Suturing of conjoint tendon with cooper’s ligament c)Shouldice(Canadian) repair: all muscle layers are sutured in double breasted manner. d)Bassini repair: Conjoint tendon sutured with inguinal ligament • Laparoscopic repair HERNIORRAPHY
- 30. LICHTENSTEIN (TENSION FREE) MESH REPAIR • In conventional methods, sutures often recreates the tension that created the hernia causing pain and a higher risk of recurrence. • In Lichtenstein repair, polypropylene mesh is used. • Overtime, due to ingrowth of tissue , the mesh safely becomes incorporated into muscle layer, creating a very strong permanent repair.
- 31. LAPROSCOPIC HERNIA REPAIR • Laproscope is inserted intraperitoneally or extraperitoneally, by making small incisions, and the abdominal contents are pulled inwards. • Mesh is placed behind the fascia tranversalis/peritoneum.
- 32. OTHER INGUINAL CANAL DEFECTS
- 33. PATENT PROCESSUS VAGINALIS PPV may lead to: 1.Indirect Inguinal Hernia 2.Hydrocele of spermatic cord and/or testis 3.Cyst
- 34. CRYPTORCHIDISM (UNDESCENDED TESTIS) • A condition in which one or both of the testes fail to descend into the scrotum from abdomen. • It may lead to compression of illio- inguinal nerve.
- 35. ENTRAPMENT OF NERVES 1)Illioinguinal nerve • Due to presence of hernia, nerve gets compressed leading to numbness and tingling sensation of a)Skin of root of penis/mons pubis b)Anterior 1/3rd of scrotum/labium majus c)Superomedial part of thigh • It may also occur if it gets cut during hernial repair 2)Genital branch of genitofemoral nerve • Its compression may lead to loss of cremasteric reflex
- 36. TESTIS Abnormal presence of splenic lobule in inguinal canal • Sometimes, spleen lobules gets fused with testicular tissue, known as SPLENOGONADAL FUSION. • Hence, the lobule will also descend into inguinal canal along with testes. SPLEENIC LOBULE
- 37. Roll no. 86 – 90 Guided By: Dr. Rajesh Astik Sir