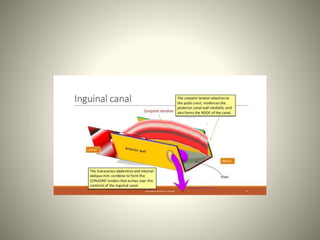
The inguinal canal is an oblique passageway in the lower anterior abdominal wall that extends from the deep inguinal ring to the superficial inguinal ring. It is approximately 3.75-4 cm long and directed downward, forward, and medially. The spermatic cord in males or round ligament in females passes through the inguinal canal. The walls of the inguinal canal include the external oblique aponeurosis as the anterior wall, internal oblique and transverse abdominis muscles forming the roof, and the inguinal ligament forming the floor. The integrity of the inguinal canal is maintained by its oblique structure as well as muscular contractions that close openings during increases