This document discusses inguinal hernia, including:
1. The surgical anatomy of the inguinal canal, its boundaries, contents, and classifications of hernias.
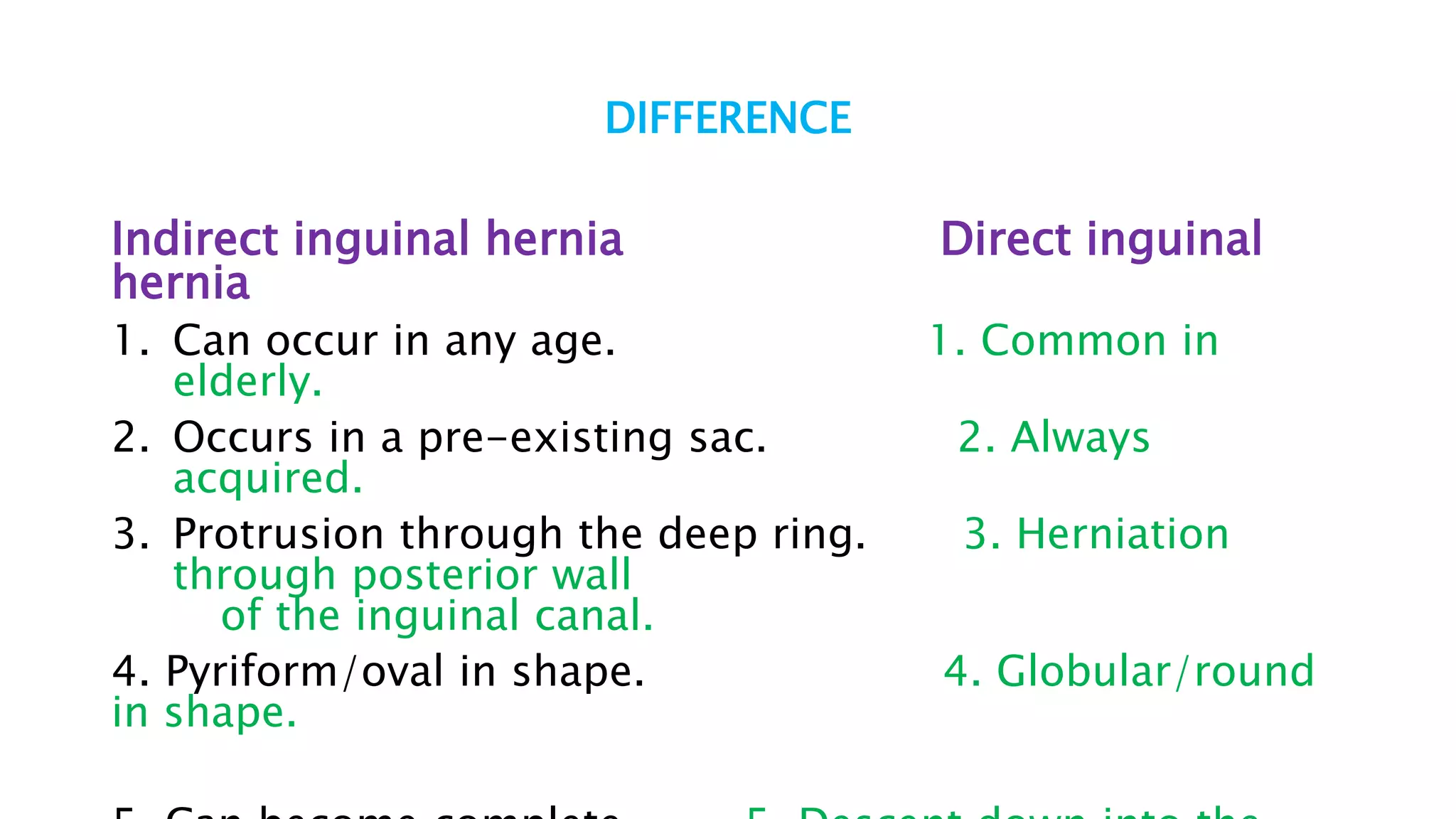
2. The differences between indirect and direct inguinal hernias.
3. Precipitating factors, clinical features, examinations, and operations for repairing inguinal hernias.