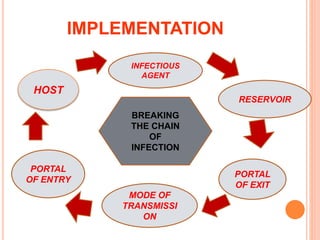
This document discusses infection prevention and standard safety measures. It begins by introducing the topic and defining hospital-associated infections. It then covers the chain of infection, types of infections like nosocomial and iatrogenic, common organisms causing infection, and the nursing process for infection control including assessment, diagnosis, goals, and implementation. It details standard, contact, airborne and droplet precautions. It concludes by discussing the roles and responsibilities of infection control nurses.
















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








