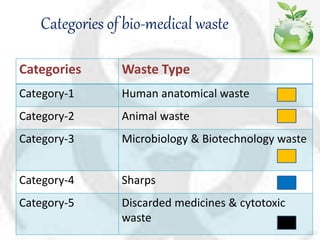
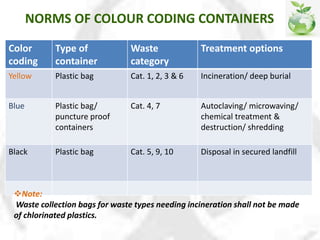
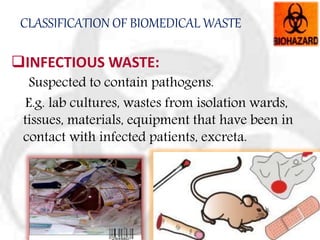
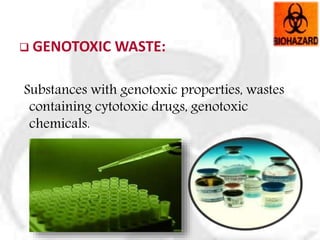
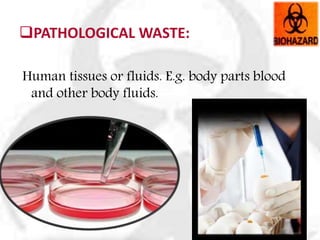
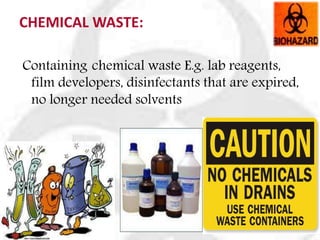
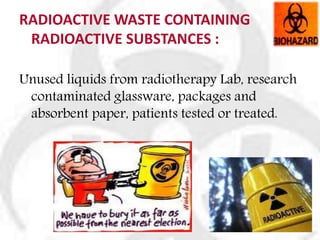
The document discusses biomedical waste management. It begins by noting the rapid increase in hospitals and disposable products has led to more medical waste. Proper waste management is important for quality assurance and public health. The document then covers waste characteristics, legislation around management, categories of waste, health hazards of improper management, and strategies for proper segregation, storage, transportation, treatment and disposal of biomedical waste.











































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












