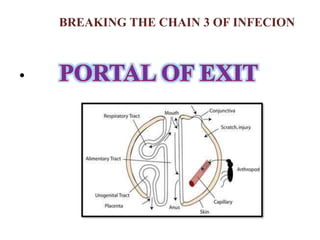
This document discusses infection control and prevention in a hospital setting. It begins by defining infection and listing some common infectious agents. It then discusses the importance of infection control in hospitals, noting that hospital-acquired infections are a leading cause of preventable death. The document outlines the chain of infection and various ways to break the chain, including appropriate handling of infectious materials and waste, sterilization and disinfection, isolation protocols, and other infection prevention strategies. It provides details on standard precautions like hand hygiene, personal protective equipment, and maintaining a sterile field during procedures. The role of nurses in infection control is also highlighted.