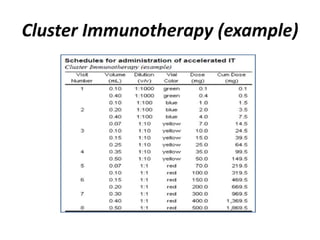
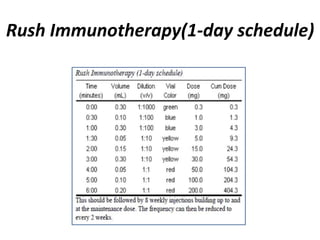
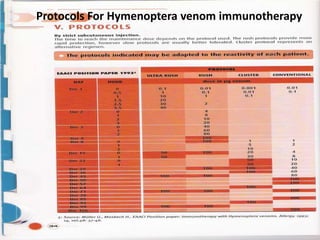
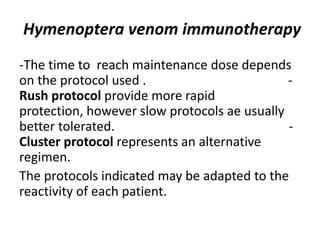
This document discusses various aspects of immunotherapy for allergies. It provides background on immunotherapy and describes different types, including subcutaneous, sublingual, oral, inhalation, and nasal immunotherapy. It discusses tests used for allergic patients like skin prick tests and RAST. It covers determining maintenance doses, benefits of immunotherapy, potential adverse reactions, and elements of informed consent. It also describes accelerated schedules like cluster and rush immunotherapy and their risks compared to standard schedules.

![Elements of Informed Consent
• Any medication (including beta-blockers) or health contraindications (eg, loss of
asthma control) should be identified.
• Duration of treatment and symptom control should be discussed.
• Patients who become pregnant while on immunotherapy may continue treatment;
however, commencing immunotherapy in pregnant women is not advisable.
Some authors do not advance immunotherapy in pregnant women until the
postnatal period.
• Subcutaneous immunotherapy should be initiated only in patients willing and
able to comply with weekly injections for a year or longer. Once maintenance is
reached, the injection regimen may become less frequent; however, several years’
duration is commonly required for clinical efficacy.
• Sublingual immunotherapy is appropriate for patients who are unable to commit
to weekly injections or those who do not want injections.
• Interestingly, a 2013 study by Kiel et al demonstrated that long-term adherence
favored subcutaneous immunotherapy over sublingual immunotherapy.[30]](https://image.slidesharecdn.com/immunotherapy-workshop-150414154248-conversion-gate01/85/Immunotherapy-workshop-14-320.jpg)















































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)