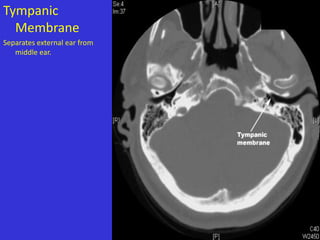
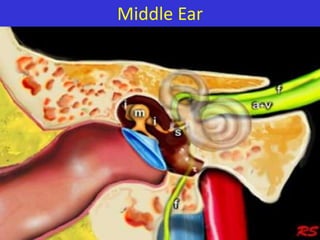
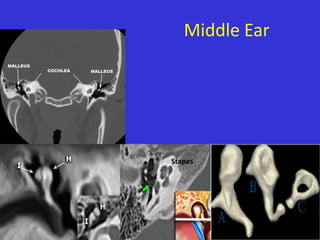
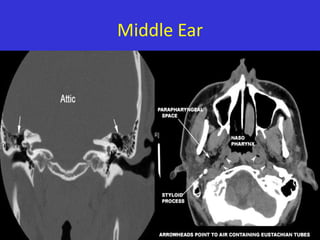
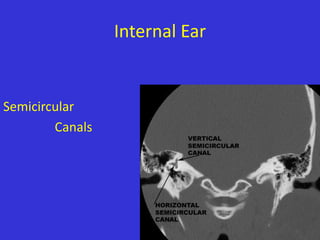
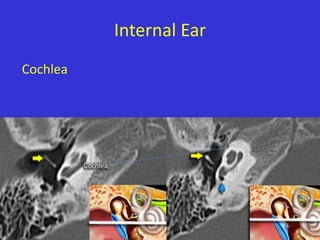
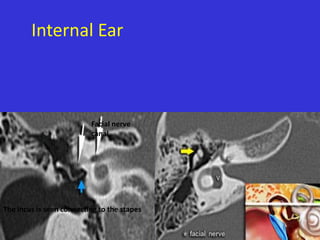
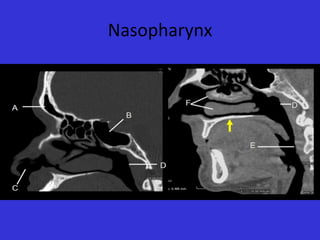
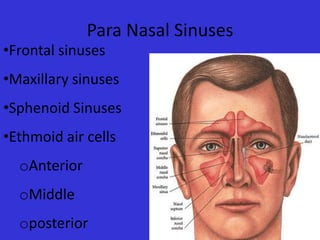
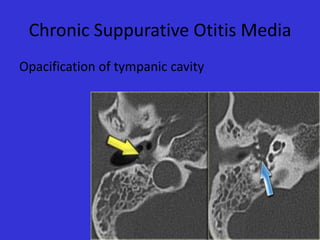
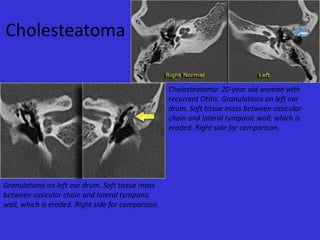
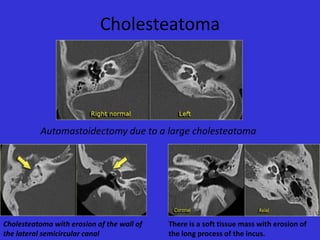
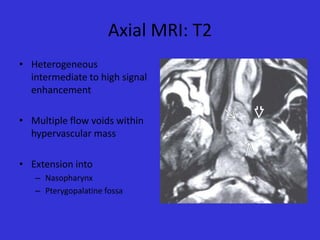
This document provides an overview of imaging modalities used in ENT and summarizes the anatomy and common diseases seen in the ear, nose, paranasal sinuses, and throat. It describes the basic anatomy of the external, middle, and inner ear. Common ENT diseases discussed include chronic suppurative otitis media, cholesteatoma, otosclerosis, deviated nasal septum, sinus polyps, and juvenile angiofibroma. Imaging findings for various diseases are presented along with anatomical images.


























































![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)































































