Downloaded 407 times


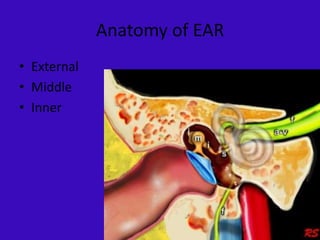













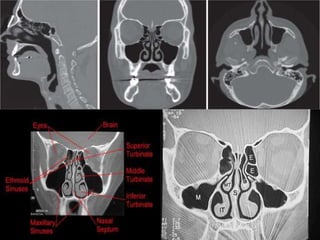

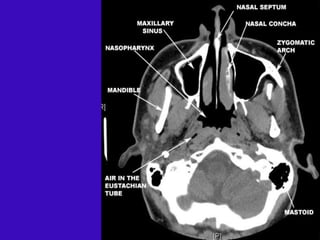
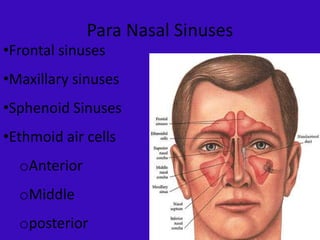









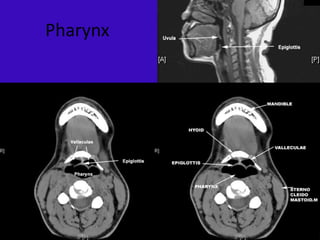




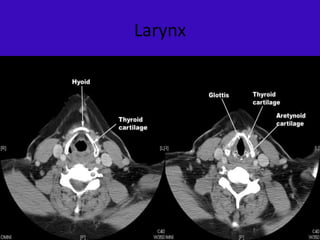










































This document provides an overview of imaging modalities used in ENT and summarizes the anatomy and common pathologies of the ear, nose, sinuses, and throat. It discusses the basic anatomy of the ear including the external, middle, and inner ear. Common ENT pathologies are described such as chronic otitis media, cholesteatoma, otosclerosis, deviated septum, sinus polyps, and angiofibroma. Imaging findings of these conditions on modalities like CT and MRI are shown. The anatomy and diseases of the nose, sinuses, throat are also reviewed.










































































































