4. HOW TO READ A X RAY
■ Type – plain/contrast
■ View – AP/lateral
■ Region – mastoid/PNS/neck
■ Identify normal landmarks
■ Identify the pathology – opacity/mass/bone destruction
5. VIEWS IN ENT X RAYS
■ EAR AND MASTOIDS – Laws view
Schullers view
Townes view
Submentovertical view
■ NOSE AND PNS – Caldwell view
Waters view
6. LAWS VIEW
■ Lateral view mastoid
■ X ray beam propelled 15
degree cephalocaudal
■ Can study mastoid air cells,
sinus plate, TM joint
■ Cant see well attic, aditus,
antrum as two side mastoid
superimpose
7. SCHULLERS VIEW
■ Lateral oblique view of
mastoid
■ X ray beam propelled 30
degree cephalocaudal
■ Separate for right and left
mastoid
■ Structures seen – mastoid air
cells, EAC, dural plate, sinus
plate, sino dural angle, TM
joint, aditus, attic, antrum
8. TOWNE VIEW
■ AP view of skull
■ Both the temporal bones
can be seen and compared
with one another
■ IAC, petrous pyramid,
arcuate eminence, sup scc,
cochlea
■ Acoustic neuroma
9. WATERS VIEW
■ AP view of PNS
■ Occipito mental view
■ Nose chin view
■ Nose and chin touch the film
■ X ray beam from occipital
side
■ Open mouth – to examine
sphenoid sinus
10. CALDWELLS VIEW
■ Occipito frontal view or
nose forehead view
■ Nose and forehead touch
the film
■ Best for frontal sinus
■ Sup margins of orbit
■ Ethmoidal sinus, maxillary
sinus
11. SOFT TISSUE OF NECK
■ Lateral view
■ Post tongue, hyoid bone,
epiglottis, tracheal shadow,
prevertebral space, cervical
vertebra
13. COMMON RADIOLOGICAL
ABNORMALITIES
■ Air-fluid levels suggest an acute process
■ Opacification = secretions, polyps, etc.
■ Thickened mucosa (check lateral maxillary wall):
Suggests chronic inflammation
■ Maxillary sinus retention cysts – Very frequent finding
■ Frontal sinus mucocele – Nasofrontal duct obstruction–
Look for loss of scalloped edge
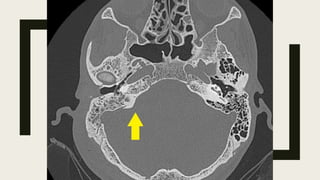
14. ACUTE OTOMASTODITIS
• CT – Investigation of choice
• partial-to-complete opacification of the mastoid air
cells.
• erosion of mastoid air cell bony septa, which
establishes the diagnosis of coalescent mastoiditis
• erosion of the lateral wall of the mastoid, suggestive
of subperiosteal abscess, or of the sigmoid plate,
suggestive of epidural abscess
16. DEVIATED NASAL SEPTUM
■ Deviated nasal septa are commonly associated
with concha bullosa or turbinate hypertrophy with
septal deviation being towards the contralateral side.
■ Nasal septal deviation can be C-shaped, reverse C-
shaped, S-shaped or reverse S-shaped
17. ACUTE SINUSITIS
■ Plain radiograph
■ Opacification of the sinuses and
level best seen in the maxillary
does not allow assessment of
the inflammation and its
Ethmoidal and sphenoidal
difficult to assess on plain
18. ■ CT FINDINGS
• peripheral or central mucosal thickening
• gas-fluid levels in the paranasal sinuses
• gas bubbles within the fluid / bubbly secretions
• obstruction of the ostiomeatal complexes.
19. CHRONIC RHINOSINUSITIS
■ The radiological features are Bone sclerosis
and demineralization can occur simultaneously
in the setting of chronic sinusitis 1. Bony
changes of chronic sinusitis include decreased
sinus size, hyperostosis and occasionally bone
demineralization if there is associated
pathology like fungal infection and sinonasal
polyposis.
20. SINONASAL POLYPS
■ extensive mucosal polyps occupying
and obliterating the nasal cavity and the
paranasal sinuses
■ associated local benign bone
remodeling or erosion (as opposed to
a mucocele where the entire sinus is
expanded 6)
21. TONSILLITIS
■ CT
• Tonsillar enlargement, which may
midline forming "kissing tonsils"
contrast images may be iso- or
• contrast enhancing linear densities
tonsils without focal fluid
• fat stranding in
22. ADENOIDS
■ The lateral neck x-ray is the main imaging
study. The size of the adenoids is less of a
consideration than the degree to which
they encroach on the nasopharyngeal
airway.
23. RETROPHARYGEAL ABSCESS
■ On plain Radiographs, which have the
advantage of being able to be obtained with the
patient sitting, demonstrate soft tissue swelling
posterior to the pharynx
■ There is widening of the prevertebral soft tissue
24. ■ CT
■ Scans should be obtained with contrast to allow
differentiation of fluid collections from phlegmonous
thickening (retropharyngeal cellulitis).
■ True abscess will usually have a peripherally
enhancing rim with a centrally hypodense collection,
expansion of the retropharyngeal space, and may
contain locules of gas
25. ACUTE EPIGLOTITIS
■ Lateral soft tissue radiograph of the neck
demonstrates thickening of the epiglottis and
aryepiglottic folds referred to as the thumb
sign.
■ It should be noted that an omega epiglottis,
either a variant of normal or in the setting
of laryngomalacia, can result in a similar
appearance and can be mistaken for
epiglottitis.
26. ■ CT is only rarely obtained, and usually when the diagnosis is unclear.
■ Indeed, placing the child in the supine position can actually precipitate
respiratory arrest. If a scan is obtained, marked edema and thickening of the
epiglottis and aryepiglottic folds may be seen with narrowing of the airway.
27. CROUP
■ Plain radiographs are not always required, as the diagnosis is
often made clinically. They are usually obtained to exclude other
causes of a similar presentation. Typical radiographic findings
include:
• steeple sign (also known as "wine bottle sign" and "inverted V
sign"): seen on AP radiographs of the neck or chest and neck
demonstrates uniform narrowing of the subglottic airway
• lateral radiograph of the upper airway will show a normal
epiglottis and narrowing of the subglottic region
28. FOREIGN BODY IMPACTION
■ A chest x-ray may help identify the
object and its location .
■ Flat things like coins or disk batteries
usually appear round on the frontal x-
ray view and flat on lateral x rays
■ Bone and glass may be detectable