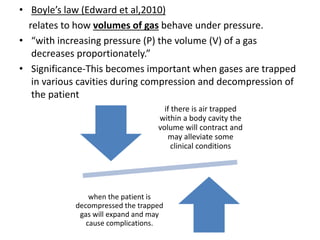
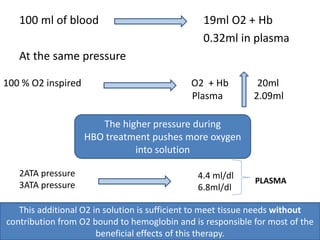
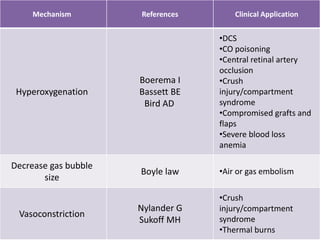
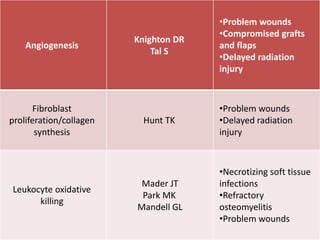
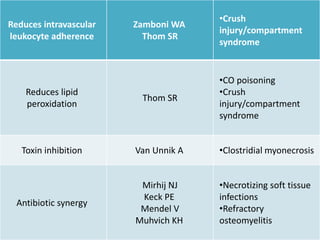
Hyperbaric oxygen therapy (HBOT) involves breathing 100% oxygen in a pressurized chamber above 1 atmosphere. HBOT increases the amount of oxygen dissolved in the blood plasma, allowing greater oxygen delivery to tissues. It has been used since the 17th century to treat various conditions and was established as a treatment for decompression sickness in the 1930s. HBOT works by increasing oxygen to tissues through hyperoxygenation and decreasing bubble size through increased pressure. It has multiple mechanisms of action including vasoconstriction, angiogenesis, and collagen formation.

![• Fick’s law (Edward et al,2010)
describes the rate of diffusion of a gas through tissues or
fluids.
• “the gas flow (volume of gas per unit time [Vgas]) through a
tissue or membrane is equal to the area (A) divided by the
thickness (T) multiplied by the diffusion constant (D) times the
difference in partial pressures (P1–P2) of the gas across the
tissue or membrane.”
• The diffusion constant is proportional to the solubility of the
gas (Sol) divided by the square root of the molecular weight
(MW) of the gas.
Vgas =D(P1 - P2)](https://image.slidesharecdn.com/seminar4-180801155156/85/HYPERBARIC-OXYGEN-THERAPY-HBOT-16-320.jpg)