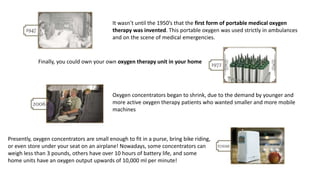
The document discusses the importance of oxygen therapy, tracing its historical development from its discovery in the 18th century to modern portable oxygen concentrators. It details the physiology of oxygen delivery, types of hypoxia, and various methods for detecting hypoxemia, emphasizing the relationship between oxygen levels in blood and tissue. The session aims to cover indications for oxygen therapy, techniques for administration, and potential complications such as oxygen toxicity.







































































![Oxygen therapy devices [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/oxygentherapydevicesautosaved-170806143146-thumbnail.jpg?width=640&height=640&fit=bounds)



















































