Downloaded 49 times
![HYPERBARIC OXYGEN Therapy [HBOT]
3
• Hyperbaric oxygen therapy(HBOT) is defined as
administration of 100% oxygen to a patient placed
inside a chamber pressurized to greater than 1
atmosphere.
• Hyperbaric oxygen exposure(breathing O2 at
increased ambient pressure, typically 2 to 3 ATA)
causes an increase in arterial and tissue partial
pressure of oxygen with no significant change in
arterial pH and partial pressure of CO2.](https://image.slidesharecdn.com/hbo-210708165604/85/Hyperbaric-oxygen-therapy-Anaesthesia-3-320.jpg)
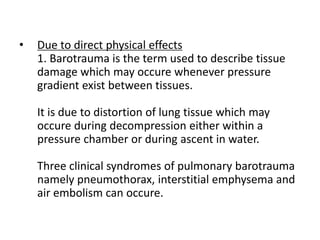
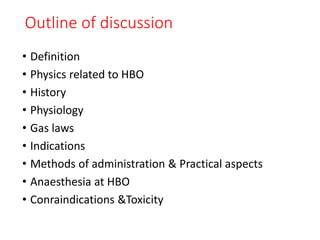
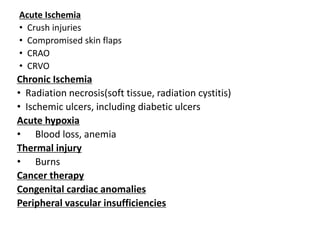
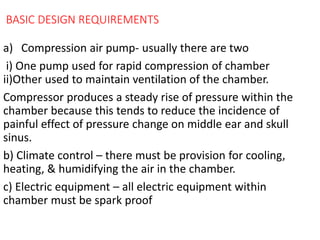
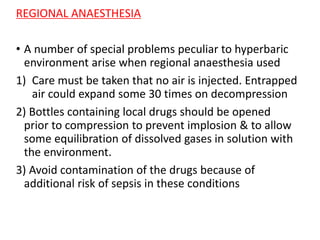
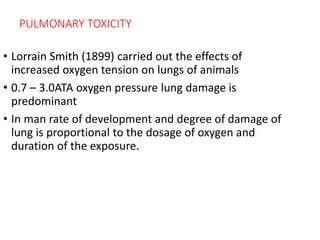
![PAO2 is 100 mm Hg at atmospheric pressure
Alveolar gas equation
PAO2 = FiO2[PB-PH2O] – PACO2
R
= 0.21[760-47] - 40
0.8
= 149.7 – 50
PAO2 = 100 mm Hg
So in HBO ,patient breathing FiO2 of 0.4 at 3 atm
3x 760 = 2200 mm Hg
• PAO2 = 0.4 x (2200 mm Hg – 47 mmHg) - 40
0.8
PAO2 = 811 mm Hg
• So increase O2 carrying capacity and increase tissue
oxygenation for the treatment of ischemic conditions.](https://image.slidesharecdn.com/hbo-210708165604/85/Hyperbaric-oxygen-therapy-Anaesthesia-25-320.jpg)



Hyperbaric oxygen therapy (HBOT) involves breathing 100% oxygen inside a pressurized chamber above 1 atmosphere. This increases the amount of oxygen dissolved in the blood and tissues. HBOT is used to treat conditions like carbon monoxide poisoning, gas embolism, necrotizing soft tissue infections, and radiation injuries by increasing oxygen delivery to compromised tissues. It works by increasing the partial pressure of oxygen inhaled, allowing more oxygen to enter the bloodstream both bound to hemoglobin and dissolved in plasma. This boosts oxygen levels in tissues to help fight infections and promote healing.
















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















