Download to read offline


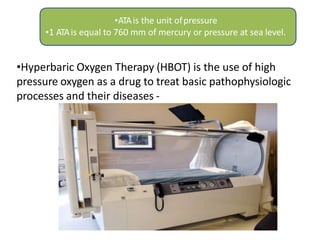




























Hyperbaric oxygen therapy (HBOT) involves breathing 100% oxygen in a pressurized chamber above 1 atmosphere. It increases the amount of oxygen dissolved in the blood plasma, which can help treat conditions like carbon monoxide poisoning, gas gangrene, non-healing wounds, and radiation injuries. HBOT works by promoting collagen formation, angiogenesis, antibiotic synergy, and inhibiting toxins and bacteria. It is used in dentistry to treat osteoradionecrosis, osteomyelitis of the jaws, aggressive periodontitis, and for dental implants in irradiated jaws by increasing oxygen levels and promoting healing. Potential side effects include oxygen toxicity, changes in vision, barotrauma, and pulmonary changes



































































