Downloaded 143 times

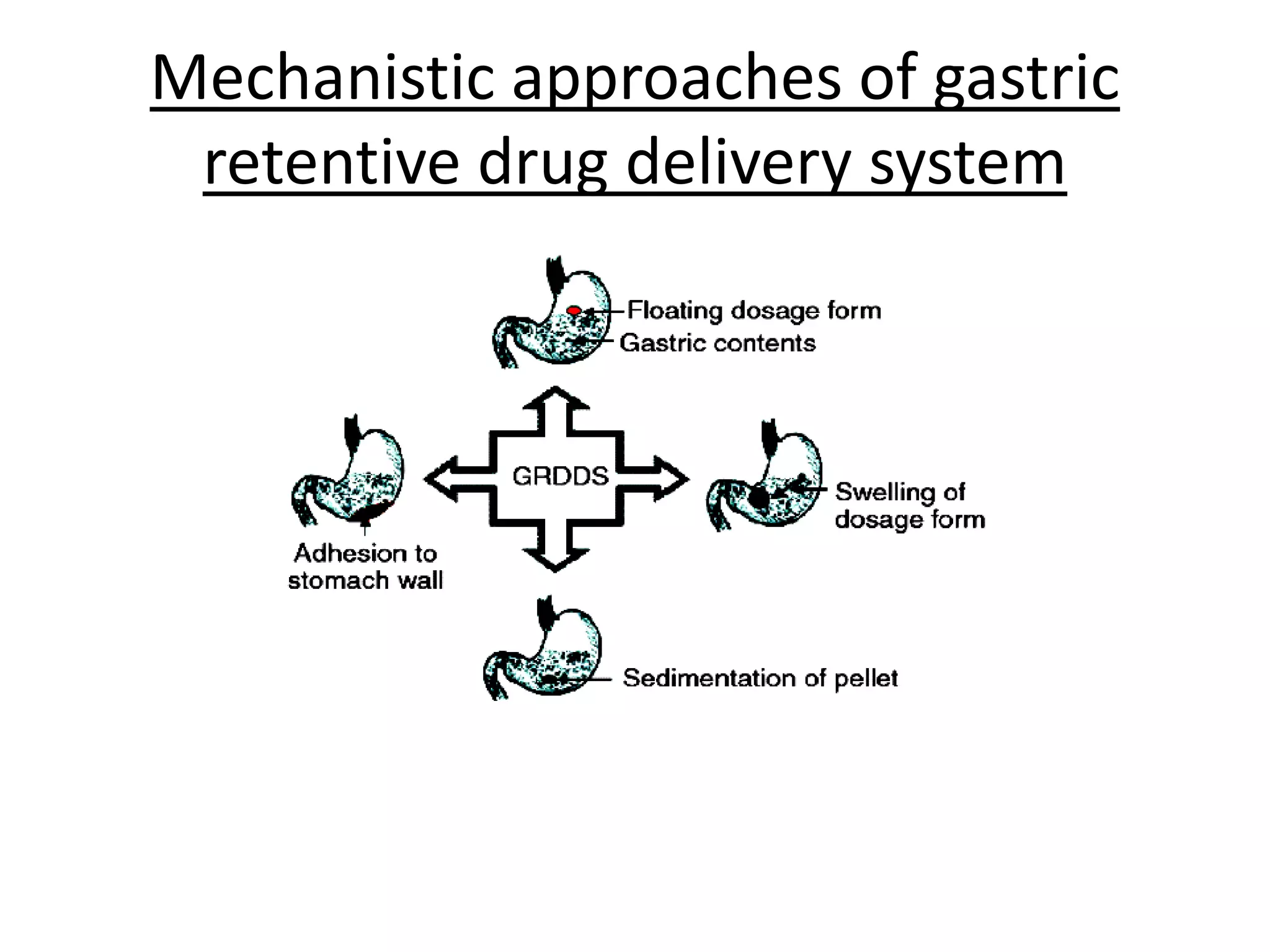
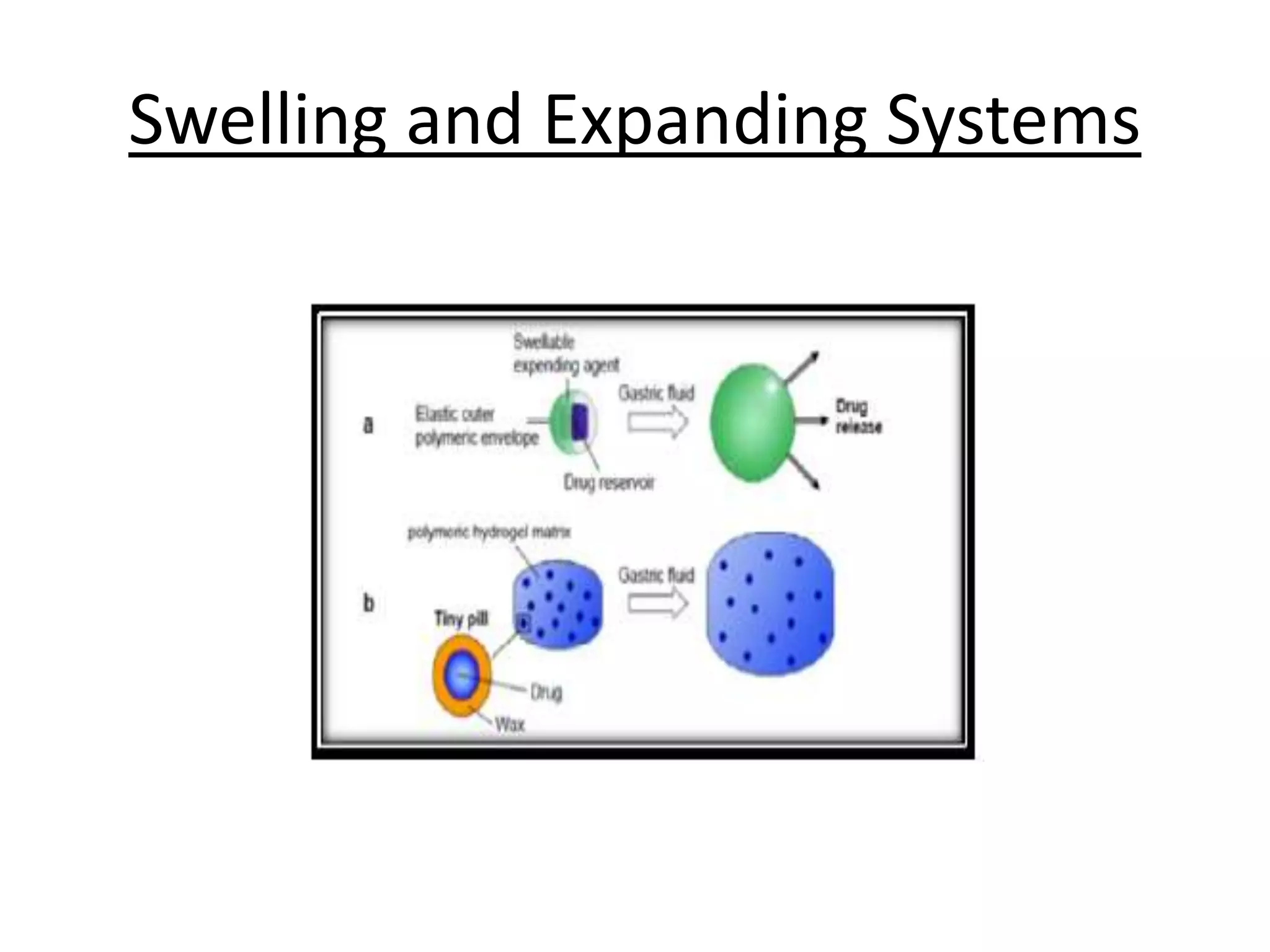
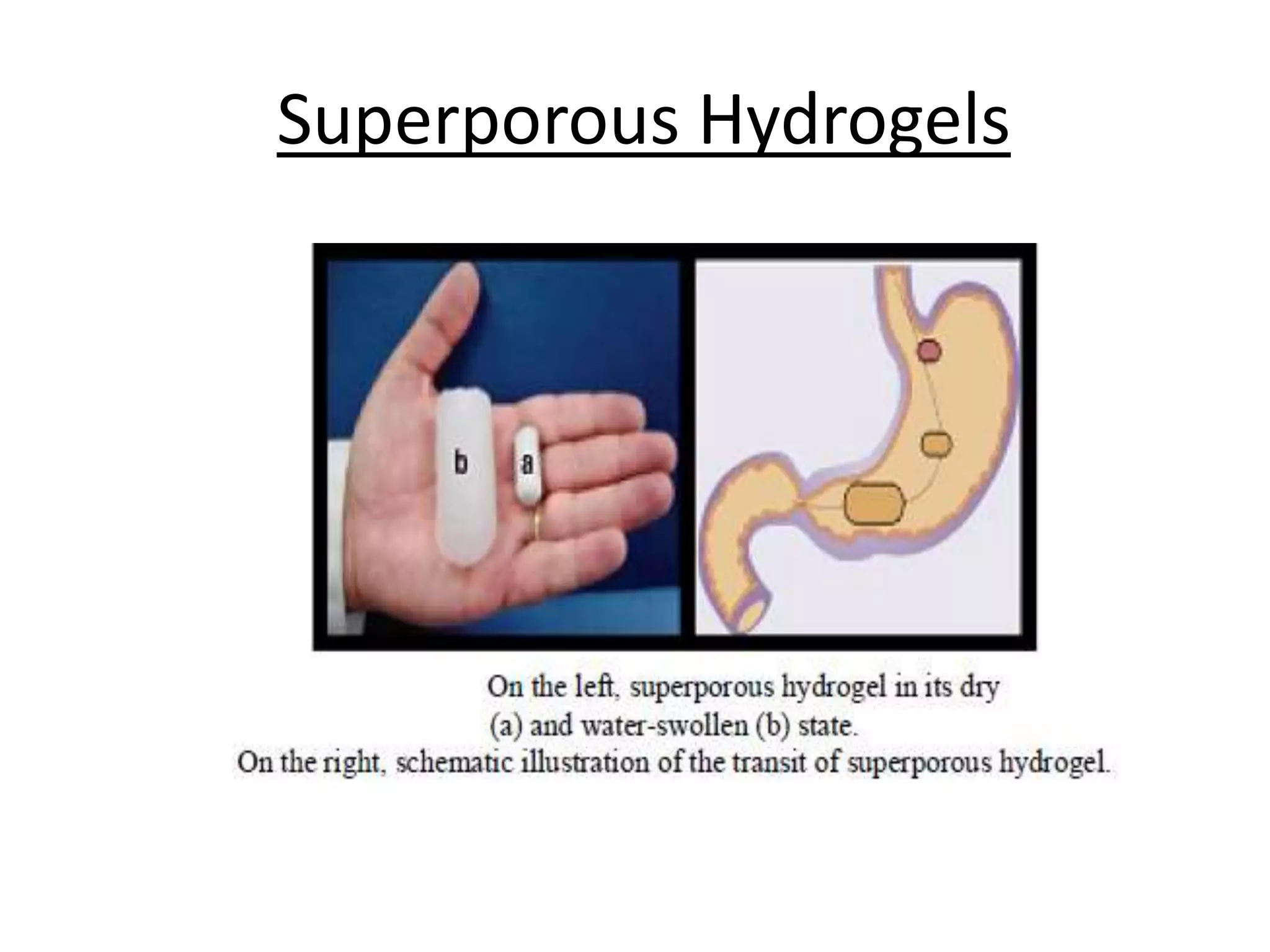

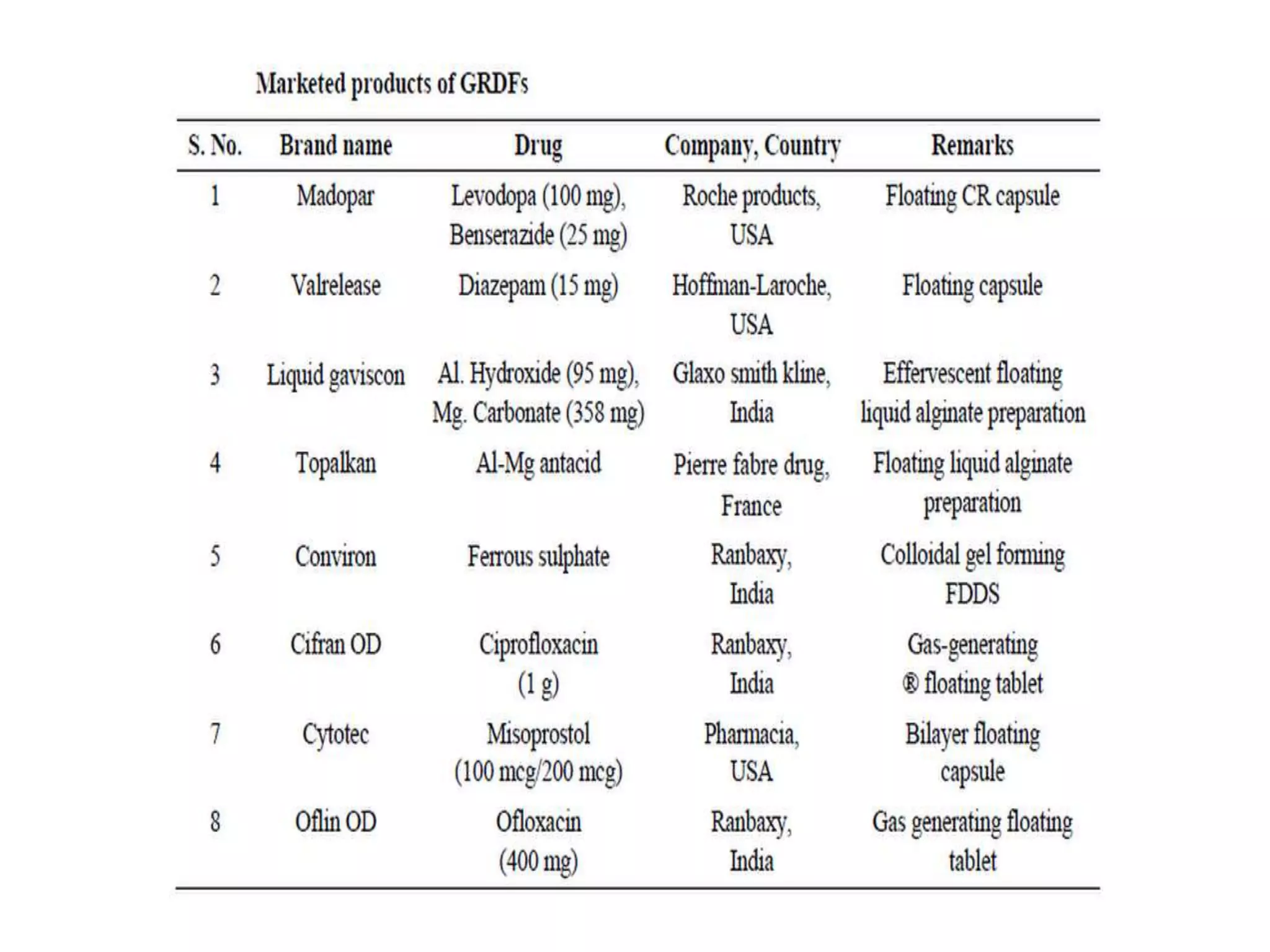

This document discusses approaches to controlled release oral drug delivery systems using hydrodynamically balanced systems. It describes various gastrointestinal anatomy and physiology factors that influence gastric retention time such as size, density, and food intake. Several mechanistic approaches to achieve prolonged gastric retention are outlined, including high-density systems, bioadhesive systems, swelling and expanding systems, magnetic systems, superporous hydrogels, and floating systems. Floating drug delivery systems that form rafts or generate gas are described as important approaches to obtain sufficient drug bioavailability through gastric retention.













































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









