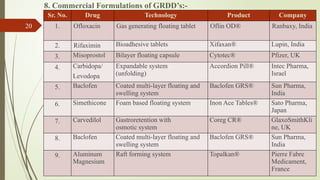
The document discusses gastro retentive drug delivery systems (GRDDS), which aim to prolong the retention time of oral drug formulations in the stomach to improve drug bioavailability and reduce dosing frequency. It outlines the advantages and disadvantages of GRDDS, various approaches for their development, and compares them with conventional drug delivery systems. The presentation, by Mr. Ravindra Popat Mali and Dr. Javesh Kashinath Patil, was part of the 4th International Online-Conference on Nanomaterials held in May 2023.
![1. Introduction:-
Drug delivery via the oral route is one of most preferred route in
state of patient compliance among the other routes. The absorption window is
the influential parameters due to which most commercially available modified
release dosage forms are acting in this physiological region for their desired
effect.
Gastro Retentive Drug Delivery System’s (GRDD’s) aims to
hold the dosage form in this stomach to attain desired activity by the formulator
against the challenges involved with the body. Improvised Control Drug
Delivery System(CDD’s) before reaching its site of absorption as compared to
conventional drug delivery, GRDD’s comparably prevails in this process of
sustaining in the GI tract influenced by the nature of excipients driven by the
type of formulation to attain therapeutic goal. Solid oral dosage forms are the
on leading class of preferred modified release system in action which
minimizes the frequency of dosing on an account to minimize multiple dosing
to attain this desired release profile [1].
3](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-3-320.jpg)
![2. Need & Rationale:-
Oral route has numerous challenges, unpredictable gastric emptying rate, a brief
gastrointestinal transit time (8-12 Hrs.), every drug candidate have its absorption window
in GIT, solubility aspects, pH dependent factors, stability, physiological region etc.
Contributing to barriers of this system still numerous products have been produced on this
account.
These difficulties have prompted researchers to design a drug delivery system which can
stay in the stomach for prolonged and predictable period. Attempts are being made to
develop a drug delivery system which can provide therapeutically effective plasma drug
concentration for a longer period, reducing the dosing frequency and minimizing
fluctuation in plasma drug concentration at steady state by delivering the drug in a
controlled and reproducible manner. One novel approach in this area is GRDDS’s. Dosage
forms that can be retained in the stomach are called GRDDs. GRDDSs can improve the
controlled delivery of drugs that have an absorption window by continuously releasing the
drug for a prolonged period of time before it reaches its absorption site [2].
4](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-4-320.jpg)
![3. Advantages:-[2, 3, 4]
Drug delivery with narrow absorption windows in the area of the small intestine.
A longer residence time in the stomach may be beneficial for local effect in the upper part of the small intestine.
E.g. to treat peptic ulcer disease.
Drugs that are easily absorbed after release in the gastrointestinal tract, such as cyclosporine, captopril, ranitidine,
amoxicillin, ciprofloxacin, etc., are expected to improve their bioavailability.
Compliance is achieved through treatment once a day.
Reduces the frequency of administration.
Targeted treatment for local disease of the upper digestive tract.
The bioavailability of therapeutic drugs can be significantly improved especially drugs metabolized in the upper
GIT by this gastro retentive drug delivery method compared to administration of non-gastro retentive drugs.
Gastric retention drug delivery can produce prolonged and sustained release of drugs from dosage forms for local
treatment in the stomach and small intestine.
Therefore, they can be used to treat diseases related to stomach and small intestine.
The drug delivery of gastric retention can minimize the side effect of human body, thereby improving the
efficiency of the drugs.
Extend the retention time of the dosage form at the absorption site.
Excellent accessibility.
Due to first pass metabolism, drug bioavailability increases.
By slowly releasing the drug at a controlled rate, drug minimized mucosal irritation.
5](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-5-320.jpg)
![4. Disadvantages:-[2, 3, 4]
Need to increase the level of gastric juice.
Not suitable for the following drugs: Problems with solubility in gastric juice,
Causing G.I stimulation, Inefficient in acidic environment.
Drugs intended for selective release in the colon.
Due to the constantly updated state of gastric mucus wall lead to unpredictable
compliance.
Hydrogel based swelling system require longer time to swell.
After multiple administrations, the increased size of the drug delivery systems
poses a threat to life due to the potential danger of permanent retention in stomach.
Super porous systems have disadvantages such as problematic storage of easily
hydrolyzed, biodegradable polymers.
Drugs that absorb equally well through GIT. E.g. Isosorbide dinitrate, Nifedipine.
Floating drug delivery systems require high fluid level in stomach to float and work
effectively.
6](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-6-320.jpg)
![5. An Overview of Gastro Retentive Drug Delivery System:-
Oral route has been the most important route of drug delivery route because of its easiness of
administration, low cost of therapy, patient compliance and flexibility in its formulation. But drugs that
are simply absorbed from gastrointestinal tract (GIT) and have short half-life are quickly eliminated
from the systemic circulation. Frequent dosing of these drugs is required to achieve suitable
therapeutic activity.
To avoid this limitation gastro retentive novel drug delivery system has been introduced.
The main benefits of gastro retentive drug delivery systems include improved bioavailability, which
leads to dosage reductions and eventually a reduction in GI disorders. They also include particular sites
for drug administration for gastrointestinal ailments. One of them is creating dosage formulations with
mucoadhesive properties. Gastric mucosal adhesion, a phenomena where the medicine attempts to mix
with stomach mucosa, is the main strategy for overcoming issues with gastric emptying time [3].
To formulate a site specific orally administered controlled release dosage form, it is desirable to
achieve a prolong gastro residence time by the drug delivery. Prolonged gastric retention time in the
stomach could be advantageous for local action in the upper part of the small intestine e.g. treatment of
peptic ulcer.
In recent year, oral dosage forms for gastric retention have drown more and more attention for their
therapeutic advantage in permitting command over the time and site of drug release. Many drugs
categorized as once a day delivery have demonstrated on transit time of dosage form. Therefore, a
system designed for longer gastric retention will extend the time within which drug absorption can
occur in small intestine [2].
7](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-7-320.jpg)
![Conventional Drug Delivery System Vs Gastro Retentive Drug Delivery System:-[2]
Sr. No. Parameters Conventional DD’s GRDD’s
1. Toxicity High risk of toxicity Low risk of toxicity
2. Patient Compliance Less Improves patient
compliance
3. Drug with narrow absorption
window in small intestine
Not Suitable Suitable
4. Drugs having rapid absorption
through GIT
Not much
advantageous
Very much
advantageous
5. Drug which degrades in the
colon
Not much
advantageous
Very much
advantageous
6. Drugs acting locally in the
stomach
Not much
advantageous
Very much
advantageous
7. Drugs which are poorly soluble
at an alkaline pH
Not much
advantageous
Very much
advantageous
8. Dose dumping High risk of dose
dumping
No risk of dose
dumping
8](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-8-320.jpg)
![Anatomy and Physiology of Gastrointestinal Tract:-[1, 2, 5, 6]
Figure 1 Anatomy of the Stomach
9](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-9-320.jpg)
![Anatomy & Histology of Stomach:-[5, 6]
Stomach has four main regions,
1) Cardia 2) Fundus 3) Body & 4) Pyloric,
Cardia is located on superior region of the stomach projects as opening region. Further
extending downward the upper curve to the left of the cardia is called fundus which is store
of undigested material just below the fundus the central part of the stomach is called body.
The pyloric region an essential region of mixing of food in the stomach consist of the parts
pyloric antrum, pyloric canal and pylorus which connects to the duodenum. The
communication between the pylorus and small intestine happens with pyloric sphincter.
The concave region is called lesser curvature and the convex as greater curvature.
Stomach consist of 4 basic layers i.e. Mucosa, submucosa, muscular & serosa.
Mucosa layer contains surface mucosa cells, Lamina propria. Epithelial cells protrude
through lamina propria and muscularis mucosae which leads to formation of gastric glands
and when this glands arranged in an manner were pits are produced which are called as
gastric pits.
Gastric gland contains three types of exocrine gland cells, parietal cells mucus neck cells,
parietal cells & chief cells. These cells contribute to the section of gastric fluid accounts
for 2 to 3 liters .The submucosa of the stomach.
10](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-10-320.jpg)
![Physiology of Digestion:-[2]
Mixing waves pass over stomach every 15-25 seconds. This waves are responsible for food
maceration called chyme, More vigorous mixing and this chyme and then it reaches reach pylorus, as
soon food reaches pyrolus each mixing wave periodically force 3 ml of chyme into duodenum, this
phenomena is called gastric emptying.
A series of electrical events occur during this whole process in this fasting state between stomach
and intestine every 2 to 3 hours governed by enteric nervous system called as migrating myoelectric cycle
(MMC) which has 4 phases.
Sr. No. Phases Name Functioning
1. Phase I Basal It is a quiescent period lasting from 30 to 60 minutes with no contractions.
2. Phase II Pre-burst
phase
It consists of intermittent contractions that gradually increase in intensity
as the phase progresses, and it lasts about 20 to 40 minutes. Gastric
discharge of fluid and very small particles begins later in this phase.
3. Phase III Burst
phase
This is a short period of intense distal and proximal gastric contractions
(4–5 contractions per minute) lasting about 10 to 20 minutes; these
contractions, also known as ‘‘house-keeper wave,’’ sweep gastric contents
down the small Intestine.
4. Phase IV -- This is a short transitory period of about 0 to 5 minutes, and the
contractions dissipate between the last part of phase III and quiescence of
phase I.
11](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-11-320.jpg)
![Factors Affecting Gastro Retention:-[7, 8]
Size
Shape of dosage form
Particle size
Density
Fed or unfed state
Frequency of feed
Nature of meal
Caloric content
Gender
Age
Posture
Nature of drugs
Formulation related factors (Polymer type, nature & conc. of excipients)
Single unit/multiple unit
Patient related factors (BMI, Chronic disease, Physical activity)
12](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-12-320.jpg)
![Ideal drug candidate for GRDD’s:-[7, 8]
Locally acting drugs in stomach
Drugs having narrow absorption window in GI tract
Drugs having narrow absorption window in intestine or colonic
conditions
Drugs having a low solubility in GI
Drugs those are unsuitable for GRDD’s:-[2]
Drugs that have very limited acid solubility e.g. Phenytoin etc.
Drugs that suffers instability in the gastric environment e.g.
Erythromycin, Rabeprazole, Clarithromycin, Esomeprazole etc.
Drugs intended for selective release in the colon e.g. 5-amino
salicylic acid and corticosteroids etc.
13](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-13-320.jpg)
![6. Approaches for gastro retentive drug delivery system:-[9, 10]
6.1 Pharmacological approach:
Co-administration of drugs with GI altering agents such as Ant-
muscarinic agents e.g. atropine, benztropine which delay gastric
emptying.
6.2 Physiological approach:
Use of fat derivatives e.g. Triethanolamine myristate which stimulate
duodenal or Jejunal receptors which slow gastric emptying.
6.3 Pharmaceutical approach:
Pharmaceutical approach is one of the most relevant approach used to
attain gastric retention as first two approach pose alteration to
physiology of the body and may lead to undesired consequences to
circadian rhythm of the body.
14](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-14-320.jpg)


![6.3.3 Super porous Hydrogels:
This dosage forms have polymers pore size less than 100 which rapidly causes swelling of polymer
which is primary properties of this formulation as delayed swelling may lead to premature evacuation of the
dosage form.
6.3.4 Mucoadhesive system:
This system in charge retain the dosage form by adhering in the gastric region different natural,
synthetic & semi-synthetic polymers are used for the development of muco-adhesive system. This adhesion leads
to retention in GRDD’s with the desired release profile with appropriative tailoring of the formulation.
6.3.5 Magnetic system:
This system simply implies placement of magnetic system inside the formulation variable and the other
magnetic system which will be placed above the abdomen to retain in the formulation in the gastric region to
achieve gastric residence time.
6.3.6 RAFT forming system:
RAFT forming system are preventive formulation gaining hold over gastro esophageal refluxes irritating
the esophageal region, this formulations form thick viscous layer above the gastric content restricting the
gastric contents to reach lower esophageal sphincter which provide a preventive action for GERD’s patients.
This formulation actually float on water which are either thick or thin having density lower than the gastric
contents such type of system termed as RAFT system which.
This RAFT forming system consist of Gel forming, swell able polymer, viscous gums etc. and CO2
driven system to make this polymer float over the gastric media. As soon as the formulation comes in contact
with the gastric media it forms a viscous layer of thick or thin type of jellified structure with some partial
entrapment of CO2 bubbles having reduced density forming RAFT system. This RAFT acts as a barrier
between stomach and its esophagus layers [9, 10].
18](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-18-320.jpg)
![7. Evaluation of Gastro Retentive Drug Delivery System:-[11, 12]
7.1 In Vitro Evaluation Parameters:-
Particle size and morphology
Drug entrapment study
Measurement of tablet tensile strength
Floating lag time (FLT), Total floating time (TFT), Floating strength
Swelling studies
Viscosity and Rheology
In vitro unfolding study
Ion exchange capacity, moisture content
In vitro drug release
Gel strength
Drug-excipient interaction study
7.2 In Vivo Evaluation Parameters:-
GRT and bioavailability of the drug
Various diagnostic imaging techniques including gamma scintigraphy, radiology,
gastroscopy, ultrasonography, and magnetic resonance imaging (MRI) can be applied for
in vivo evaluations of GRDD’s.
19](https://image.slidesharecdn.com/powerpoint-241126073044-a457b00e/85/GRDDS-Drug-Delivery-System-powerpoint-pptx-19-320.jpg)