
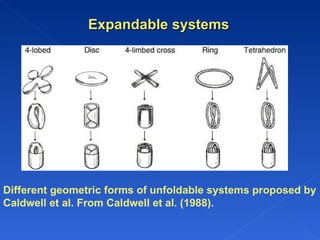
![These systems include Unfoldable and Swellable systems. Unfoldable systems are made of biodegradable polymers. The concept is to make a carrier, such as a capsule, incorporating a compressed system which extends in the stomach. Caldwell et al. proposed different geometric forms (tetrahedron, ring or planar membrane [4-lobed, disc or 4-limbed cross form] ) of bioerodible polymer compressed within a capsule. Swellable systems are retained because of their mechanical properties. The swelling is usually results from osmotic absorption of water. The device gradually decreases in volume and rigidity as a result depletion of drug and expanding agent and/or bioreosion of polymer layer, enabling its elimination.](https://image.slidesharecdn.com/sagargrddsfinalpptpd-110719112610-phpapp02/85/Sagar-grdds-final-ppt-pd-23-320.jpg)


The document discusses gastroretentive drug delivery systems (GRDDS) and their role in enhancing the bioavailability of drugs that are absorbed in the stomach or upper small intestine. It highlights the advantages and limitations of GRDDS, including suitable drug candidates and unsuitable ones for this system. Various approaches to achieve prolonged gastric retention through different mechanisms such as buoyancy, swelling, and bioadhesion are also explored.









































































