Download to read offline
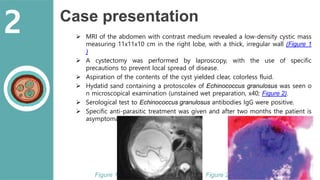

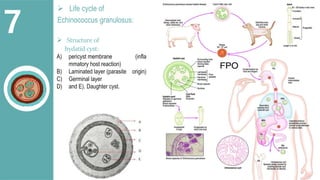


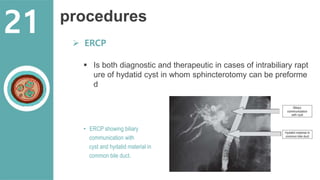

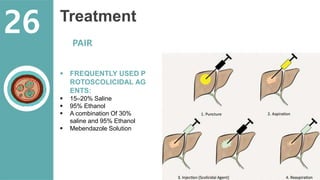


The document presents a comprehensive overview of hydatid cystic disease, focusing on a case of a 32-year-old woman diagnosed with a hydatid cyst in the liver caused by Echinococcus granulosus. It outlines the disease's etiology, clinical presentation, diagnostic workup, treatment options including medical, paired techniques, and surgical interventions, as well as prevention strategies. Key epidemiological details are provided, highlighting global prevalence and the importance of proper hygiene and veterinary measures to control the disease.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
