Downloaded 267 times


































![REFERENCES
1.Janice L. Hinkle, Kerry H. Cheever. Brunner and Suddarth’s Textbook of Medical Surgical
Nursing. 2015. New Delhi. Wolters Kluwer.13th Edition. Volume 2. Pg. no. 1349-1354.
2.Lewis. Medical Surgical Nursing Assessment and Management of clinical problems.2015.
New Delhi. Elsevier. 2nd Edition. Volume II. Pg. no.998, 1068.
3.Mayo Clinic. Oesophageal varices. Available from https://www.mayoclinic.org/diseases-
conditions/esophageal-varices/symptoms-causes/syc-
20351538#:~:targetText=Esophageal%20varices%20are%20abnormal%2C%20enlarged,scar%2
0tissue%20in%20the%20liver. [cited 8 nov 2019]
4.PubMed. Use of Wireless Capsule Endoscopy for the Diagnosis and Grading of Esophageal
Varices in Patients With Portal Hypertension: A Systematic Review and Meta-Analysis.
Available from https://www.ncbi.nlm.nih.gov/pubmed/27548729 [cited 8 nov 2019]
5.PubMed. Evaluation of the blood ammonia level as a non-invasive predictor for the
presence of esophageal varices and the risk of bleeding. Available from
https://www.ncbi.nlm.nih.gov/pubmed/30465524 [cited 8 nov2019]](https://image.slidesharecdn.com/esophagealvarices-191114153554/75/Esophageal-varices-47-2048.jpg)



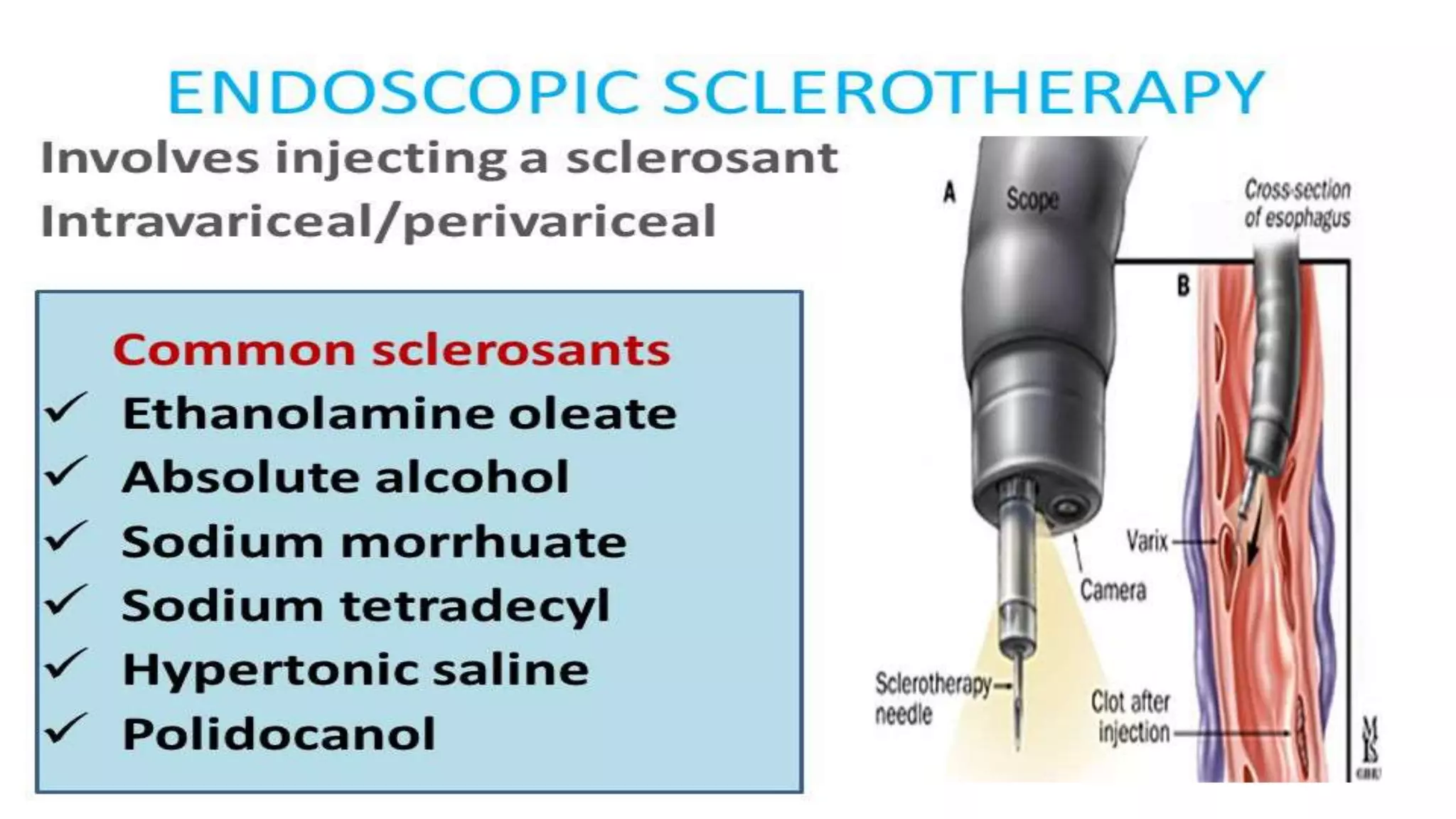
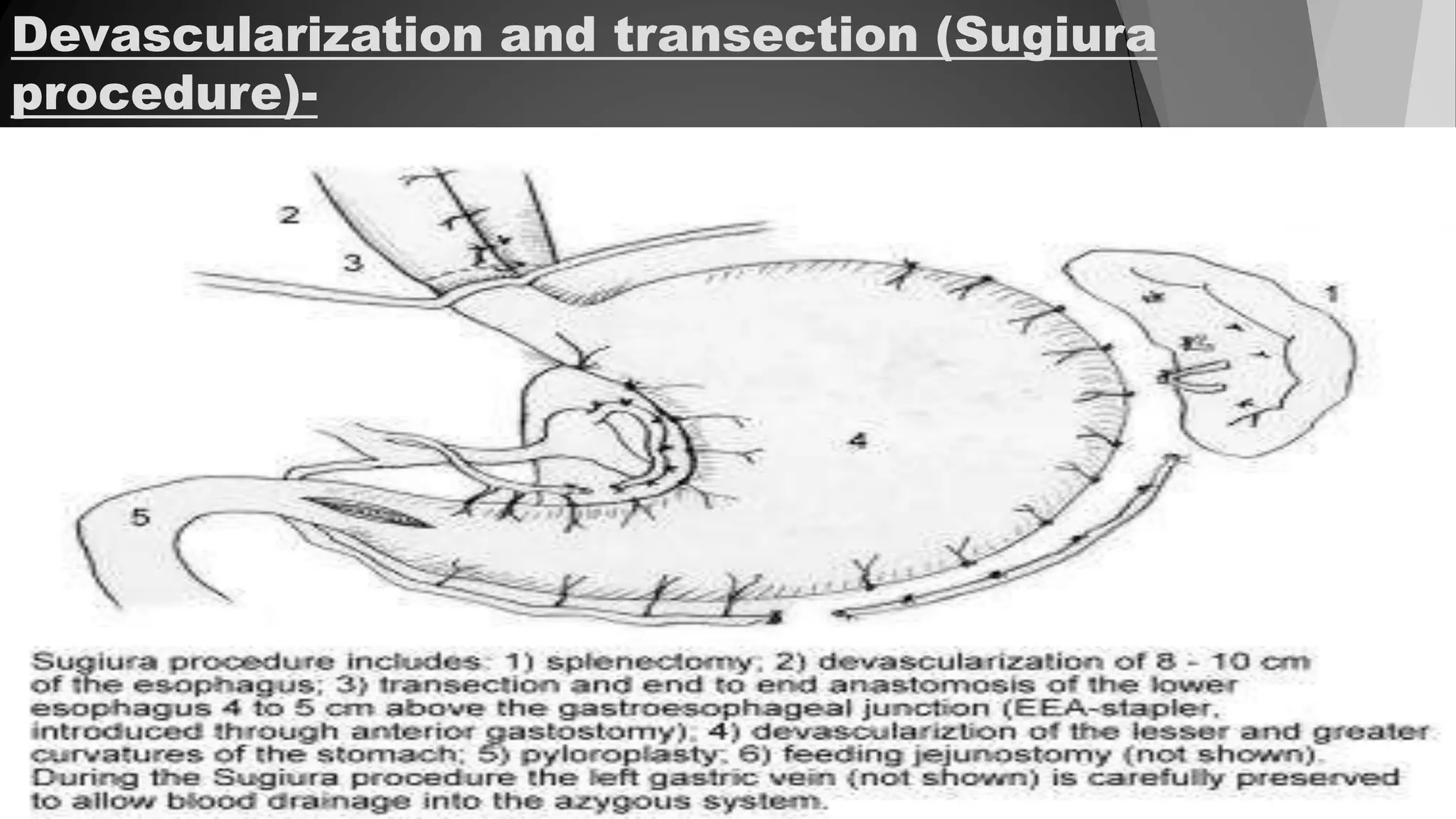
This document discusses oesophageal varices, which are dilated and tortuous veins in the oesophageal wall caused by increased venous pressure. Varices are prone to rupture and bleeding. The document defines portal hypertension and discusses the epidemiology, etiology, risk factors, pathophysiology, clinical manifestations, diagnostic evaluations, medical and surgical management, nursing care, and conclusions regarding oesophageal varices. It also summarizes two research articles on using capsule endoscopy to diagnose varices and using blood ammonia levels to predict variceal presence and bleeding risk.











































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)











