Downloaded 146 times
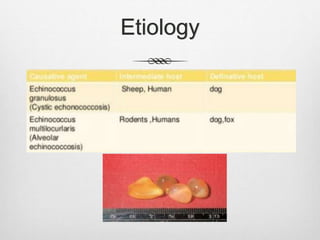






















Echinococcosis is a parasitic disease caused by tapeworms of the genus Echinococcus. There are four main species that can cause disease in humans. The most common are E. granulosus, which causes cystic echinococcosis, and E. multilocularis, which causes alveolar echinococcosis. People typically become infected by ingesting Echinococcus eggs from contact with infected dog feces. The parasites' larvae can develop cysts in organs like the liver and lungs. Symptoms depend on the location and size of cysts but may include abdominal pain or coughing. Diagnosis involves imaging tests and serological analysis. Treatment involves antiparasitic medications and potentially surgery























































































