Introduction
• Echinococcosis (hydatiddisease) is a zoonosis
caused by the larval stage of Echinococcus
granulosus (also known as Taenia echinococcus).
• Humans are accidental intermediate hosts,
whereas animals can be both intermediate and
definitive hosts.
• The 2 main types of hydatid disease are caused by
E granulosus and Echinococcus multilocularis.
3.
• The formeris commonly seen in the
Mediterranean, South America, the Middle
East, Australia, and New Zealand, and is the
most common type of hydatid disease.
• In humans, 50% to 75% of the cysts occur in
the liver, 25% are located in the lungs, and 5%
to 10% distribute along the arterial system.
Infection with echinococcal organisms is the
most common cause of liver cysts in the world.
4.
Etiology
• The lifecycle of E granulosus has 2 hosts.
– The definitive host is usually a dog or some other
carnivore.
– The adult worm of the parasite lives in the proximal
small bowel of the definitive host attached by
hooklets to the mucosa. Eggs are released into the
host’s intestine and excreted in the feces.
– Sheep are the most common intermediate host,
and these animals ingest the ovum while grazing.
5.
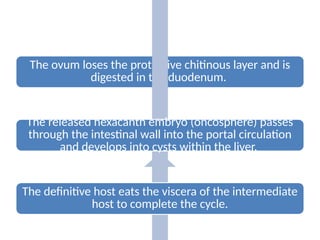
The ovum losesthe protective chitinous layer and is
digested in the duodenum.
The released hexacanth embryo (oncosphere) passes
through the intestinal wall into the portal circulation
and develops into cysts within the liver.
The definitive host eats the viscera of the intermediate
host to complete the cycle.
6.
• Humans maybecome intermediate hosts through
contact with the definitive host (usually a dog) or
by ingestion of contaminated water or vegetables.
• Once in the liver, cysts grow to 1 cm in the first 6
months and 2 to 3 cm annually thereafter.
• Once the parasite passes through the intestinal
wall into the portal venous or lymphatic system,
the liver is the first line of defense, and thus is the
most frequently involved organ.
7.
Incidence
• The incidenceof hydatid liver cysts in the United States is
approximately 200 cases per year, with an increased frequency in
immigrant populations.
• Hydatid liver disease affects all age groups and both sexes equally,
and no predisposing pathologic conditions are associated with
infection.
• Public education about the life cycle and transmission of the
disease has helped decrease the incidence.
• Washing hands after contact with canines, eliminating the
consumption of vegetables grown at ground level from the diet,
and stopping the practice of feeding entrails of slaughtered animals
to dogs have all aided in decreasing the incidence of the disease.
8.
Pathology
• Hydatid livercysts tend to expand slowly and
without symptoms and are thus frequently
very large on presentation. Single lesions are
noted in 75% of patients and are
predominantly located within the right lobe
(80%).Even though the lesion is single, half
contain daughter cysts and are multilocular.
9.
• The typicalhydatid cyst has a 3-layer wall surrounding a
fluid cavity.
• The outer layer is the pericyst,
– a thin
– indistinct fibrous tissue layer representing an adventitial reaction
to the parasitic infection.
– The pericyst acts as a mechanical support for the hydatid cyst and
is the metabolic interface between the host and the parasite.
– As the cyst grows, bile ducts and blood vessels stretch and
become incorporated within this structure. This process explains
the biliary and hemorrhagic complications of cyst growth and
difficulties with resection. Over time, the pericyst calcifies.
10.
– The outerlayer of the cyst itself is the ectocyst or
laminated membrane and is bluish-white,
gelatinous, and about 0.5 cm thick.
– This membrane is a cuticular chitinous structure
without nuclei and acts as a barrier for bacteria
and an ultrafilter for protein molecules
11.
• The innerlayer or endocyst is the germinal membrane.
– responsible for the production of clear hydatid fluid, the ectocyst, brood
capsules, scoleces, and daughter cysts.
– The endocyst is 10 to 25 µm thick and attached tenuously to the laminated
membrane.
– The absorptive function of the inner layer is important for cyst nutrition.
– The inner layer also has a proliferative function producing the ectocyst and
scoleces. This germinal layer forms smallcellular masses that give rise to
brood capsules, in which future worm heads develop.
– They enlarge and develop into invaginated protoscoleces with 4 suckers
and a double row of hooks—a protoscolex. The protoscolex fully
differentiates and matures attached by a pedicle to the capsule wall. Brood
capsules and freed protoscoleces are released into the fluid of the original
cyst and, together with calcareous bodies, form hydatid sand
12.
– Hydatid sandis made up of around 400,000 scoleces per
milliliter of fluid.
– The protoscolex can differentiate in 2 directions.
– In the definitive host, the scolex becomes an adult
tapeworm.
– In the intermediate host, including humans, each of the
released protoscoleces is capable of differentiating into a
new hydatid cyst.
– Development of brood capsules from the germinal layer
indicates complete biologic development of the cyst,
which occurs after 6 months of growth.
13.
• Daughter cystformation is a defense reaction.
• Hydatid cysts in humans are long-standing, large, and
liable to injury.
• Any injury may cause daughter cyst formation.
• Daughter cysts are replicas of the mother cyst, and
their size and number are variable.
• In uncomplicated cysts, the cyst cavity is filled with
sterile, colorless, antigenic fluid containing salt,
enzymes, proteins, and toxic substances. The formation
of daughter cysts is called endogenic vesiculation
14.
• Ectogenic vesiculationoccurs when a small rupture or defect in
the laminated membrane occurs and the germinal layer passes
through and creates a satellite hydatid cyst.
• This process is uncommon in E granulosus, but is characteristic
for the larval stage of E multilocularis.
• Because the liver parenchyma in humans cannot sequester E
multilocularis and the process of ectogenic vesiculation is
fulminant, multiple vesicles are formed in all directions. The
infected parenchyma has a multilocular appearance, and the
center becomes necrotic, spongy, and filled with a gelatinous
fluid similar to that of a mucoid liver carcinoma. Hepatic
insufficiency is common, and the disease is often lethal
15.
Diagnosis
• The diagnosisof uncomplicated hydatid liver
cyst depends on the index of clinical suspicion.
Most uncomplicated cysts are asymptomatic.
Symptoms may arise due to a toxic reaction
from the presence of the parasite or local
mechanical effects.
16.
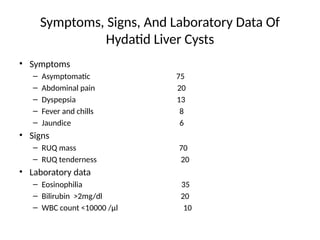
Clinical Presentation
• Itdepend on the site, size, stage of development.
• Whether the cyst is alive or dead, and whether the cyst is
infected.
• Pain in the RUQ or epigastrium is the most common
symptom, whereas hepatomegaly and a palpable mass are
the most common signs.
• Nonspecific fever, fatigue, nausea, and dyspepsia may also
be present
• Approximately one-third of patients will have eosinophilia,
and only 20% will present with jaundice and
hyperbilirubinemia.
Serology
• Enzyme-linked immunosorbentassay (ELISA)
gives a positive result in more than 90% of
patients.
• Specific IgE antibodies are demonstrated with
ELISA and radioallergosorbent test (RAST) if
active disease is present.
19.
Radiology
• Chest radiographsmay show an elevated
diaphragm and concentric calcifications in the
cyst wall.
• USG and CT are considered the first choice for
imaging.
• Classic findings of hydatid cysts are calcified thick
walls, often with daughter cysts.
• The specificity of USG in hydatid disease is
around 90%.
20.
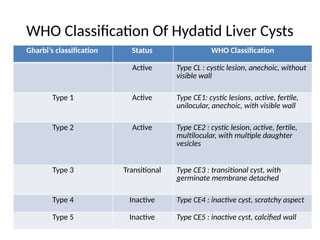
WHO Classification OfHydatid Liver Cysts
Gharbi’s classification Status WHO Classification
Active Type CL : cystic lesion, anechoic, without
visible wall
Type 1 Active Type CE1: cystic lesions, active, fertile,
unilocular, anechoic, with visible wall
Type 2 Active Type CE2 : cystic lesion, active, fertile,
multilocular, with multiple daughter
vesicles
Type 3 Transitional Type CE3 : transitional cyst, with
germinate membrane detached
Type 4 Inactive Type CE4 : inactive cyst, scratchy aspect
Type 5 Inactive Type CE5 : inactive cyst, calcified wall
21.
• MRI providesstructural details of the hydatid cyst.
• Magnetic resonance cholangiopancreatography
(MRCP) may show communication with the biliary
system as well as provide detailed information on the
biliary anatomy.
• Endoscopic retrograde cholangiopancreatography
(ERCP) or percutaneous transhepatic cholangiogram
(PTC) may show communication between the cysts
and bile ducts and can be used to drain the biliary tree
before surgery.
22.
Treatment
• Most echinococcalcysts are asymptomatic on presentation, but
potential complications such as pulmonary infection,
cholangitis, rupture, and anaphylaxis.
– Medical
– Surgical
– percutaneous approaches
• Small cysts (<4 cm) located deep in the parenchyma of the liver,
if uncomplicated, can be managed conservatively.
• Basic principles include:
– eradication of the parasite within the cyst
– protection of the host against spillage of scoleces
– management of complications
23.
Antihelminthics
• Medical therapyfor echinococcosis is based on the
benzimidazoles (mebendazole and albendazole)
and, used alone, is only 30% successful.
• Albendazole is readily absorbed from the intestine
and metabolized by the liver to an active form.
• Mebendazole is poorly absorbed and is inactivated
by the liver.
• Albendazole is thus the drug of choice for medical
therapy.
24.
• ABZ isthe only drug that is ovicidal, larvicidal,
and vermicidal and is the drug of choice.
• Praziquantel, a synthetic isoquinoline pyrazine
derivative, has been used in combination with
ABZ to increase the protoscolicidal effect of
ABZ
25.
Indication
Inoperable patientswith primary liver and lung cystic
echinococcosis,
Patients with multiple cysts in two or more organs
multiple small (<5 cm, CE1 and CE3) liver cysts
cysts deep in liver parenchyma
prevention and management of secondary hydatidosis
management of recurrent hydatidosis
unilocular cysts in unfit elderly patients
in combination with surgery and interventional procedures
pulmonary echinococcosis
long-term administration for cysts at specific sites (such as
bone, brain, eye).
26.
Contraindication
Large cysts (>10cm)
Cysts with multiple septa divisions (honeycomb like
cysts)
Cysts that are prone to rupture (superficial)
Infected cysts
Inactive cysts
Asymptomatic calcified cysts
Severe chronic hepatic disease
Bone marrow depression
27.
• According tothe WHO-IWGE guidelines,
preinterventional administration of ABZ or MBZ
should begin 4 days before intervention and
continue 1 month for ABZ and 3 months for MBZ.
• ABZ is given orally at a dose of 10 to 15
mg/kg/day, in two divided dose with a fat-rich
meal.
• The optimal treatment period ranges from 3 to 6
months.
28.
• MBZ isgiven at a dosage of 40 to 50
mg/kg/day in three divided doses with a fat-
rich meal if ABZ is not tolerated.
• Duration of therapy is also 3 to 6 months.
• Praziquantel is given at dosage is 40
mg/kg/wk.
– It has been used for the management of
intraperitoneal spillage during operative and
interventional procedures.
29.
• Monitoring foradverse effects of ABZ & MBZ
is mandatory.
– CBC count and liver enzyme determination every 3
weeks for the first 3 months, followed by repeated
determinations once a month if the therapy is
prolonged.
30.
Percutaneous Aspiration AndDrainage
• PAIR technique stands for: puncture of the
cyst wall, aspiration of cyst content, injection,
and reaspiration of a scolecidal agent.
• The most frequently used protoscolecidal
agents used for percutaneous treatment are
15% to 20% saline, 95% ethanol, a
combination of 30% saline and 95% ethanol,
and mebendazole solution.
• Complicated cysts,cysts with many daughter
cysts, or largevolume cysts are indications for
PAIR modifications:
– the PAIR catheterization technique
– the D-PAI (double-puncture, aspiration, and
injection) technique
– the percutaneous evacuation of cyst content (PEVAC)
technique
– the modified catheter aspiration technique (MoCAT).
34.
Indications for PAIRTechnique
• liver hydatid cysts are type I and II cysts.
• Type III and IV cysts with drainable material.
• Suspected fluid collections.
• Infected hydatid cysts.
• Inoperable patients –
– pregnant women.
– Patients with multiple, disseminated, or
symptomatic cysts.
35.
Contraindications for PAIRTechnique
• Type III and IV cysts (hydatid cysts with
heterogeneous echo pattern).
• Liver cysts that have ruptured into the biliary
system or peritoneum.
• Cysts inaccessible to puncture.
• Children <3 years old.
• Type V cysts are not eligible for any
intervention other than simple follow-up.
36.
SURGERY
• Surgery remainsthe treatment of choice for
uncomplicated hydatid disease of the liver.
• Objectives of surgical treatment are to:
– Inactivate the scoleces
– Prevent spillage of cyst contents
– Eliminate all viable elements of the cyst
– Manage the residual cyst cavity
37.
Open Cyst Evacuation
•Safest surgical approach
• Peripherally located cysts are the most easily treated, and either
abdominal or flank approaches may be used depending on cyst
location.
• Prior to opening the cyst, the field is lined with hypertonic (20%)
saline-soaked gauze to guard against spillage.
• The cyst is then opened, and the contents are aspirated with a
suction device that is capable of generating high negative pressures.
• The cyst is then opened completely, and any remaining debris is
meticulously cleared. The cavity may then be irrigated with a
scolecidal agent.
• The recurrence rate of this procedure is 10% to 30%.
38.
Laparoscopic Cyst Evacuation
•The lesions best suited for this approach are
situated anteriorly and do not have thick
calcified walls.
• A right lateral approach also works for cysts in
segments VI and VII
40.
Pericystectomy
• Pericystectomy involvescomplete resection of
the cyst wall without entering the cyst cavity.
• Pericystectomy decreases the risk of spillage
of cyst contents into the peritoneal cavity and
also lowers the risk of recurrence
Complications
• Most commonly,the cyst ruptures internally or
externally, followed by secondary infection,
anaphylactic shock, and liver failure.
• Viable hydatid cysts are space-occupying lesions
with a tendency to grow. In confined areas such
as the central nervous system, even small cysts
can cause severe symptoms
• In less confined areas, symptoms depend on
the site and size of the cyst.
Suppuration and SecondaryBacterial
Infection
• Cyst leakage is a prerequisite for bacterial
contamination, and the most frequent cause of
infection is a cystobiliary communication (CBC).
The clinical presentation is as a liver pyogenic
abscess.
• Occasionally, the entire cyst content undergoes
aseptic necrosis, the parasite dies, and the cyst is
filled with amorphous, yellow debris that must be
distinguished from the pus of secondary infection.
45.
Pressure Effects, Rupture,and Bile Duct
Communications
• A viable liver HC has the tendency to grow in
the direction of least resistance.
– This accounts for its frequently irregular shape.
• An enlarging cyst causes compressive atrophy
of surrounding hepatocytes and fibrosis,
which can lead to compensatory hypertrophy
of the remaining liver parenchyma.
46.
• Large cystscan replace an entire liver lobe.
• Serious consequence of cyst enlargement is
that it can rupture.
– Obscure rupture.
– Free rupture.
– communicant rupture.
47.
Obscure (Internal) Rupture
•Injury or penetration of bile into the space
between the pericyst and the endocyst can
cause rupture of the laminated membrane
• The liberated protoscoleces occupy the
available space and develop into hundreds of
daughter cysts within the pericyst cavity.
• A typical univesicular cyst becomes
multivesicular
48.
• When sucha cyst is surgically entered, there is
no laminated membrane and hundreds of
daughter cysts, floating in a yellowish fluid and
gelatin-like amorphous mass, crowd the
interior of the pericyst.
• A multivesicular cyst with viable daughter cysts
retains its high intracystic pressure, continues
to enlarge, and can damage the host
49.
• The clinicalsignificance of multivesicular cysts is
that
– the host is exposed to hydatid antigens in the hydatid
fluid
– the cyst is bacteriologically sterile
– the cyst contents cannot be easily aspirated and need
to be scooped out
– the cyst must be treated as viable and infective
– bile-stained cyst contents mandate a meticulous
search for CBC
50.
Free Rupture
• Infree rupture, the hydatid contents
disseminate throughout the peritoneal or
pleural cavity.
• There areseveral clinical presentations of intraperitoneal
rupture:
a. In acute symptomatic rupture, peritoneal irritation and acute
abdominal symptoms occur. This is an uncommon event. The
incidence is about 1% to 4%.
b. In anaphylactic shock, rupture of the hepatic HC precipitates
severe circulatory collapse, which may be fatal, and tends to
mask the abdominal manifestations.
c. In silent rupture, the patient presents with disseminated
abdominal hydatidosis, unaware when the rupture occurred.
d. Herniation of the laminated membrane (“dumbbell
hepatoperitoneal cyst”) occurs through the pericyst
53.
• Intraperitoneal ruptureis a life-threatening
complication that results in “secondary
echinococcosis.” Multiple cysts develop
throughout the peritoneal cavity, causing
intestinal obstruction, gross abdominal
distention, ascites, and cachexia.
54.
Intrathoracic Rupture
• Anelevated hemidiaphragm and a sterile
sympathetic pleural effusion can be the first
signs of liver hydatid disease.
• Upward extension of a subdiaphragmatic cyst is
usually asymptomatic, although it can cause
– Dry cough
– Dyspnea
– chest pain
– toxemia
55.
• The pleuraand adherent basal lung segments
often become inflamed and indurated. Frank
intrapleural rupture with empyema
(hydatopiothorax) is rare.
• A combination of infection and pressure can
cause destruction of lung parenchyma, resulting
in pneumonitis or lung abscess.
• A HC may erode into a bronchiole and the
contents can be evacuated.
56.
• Rupture intothe lumen of a bronchiole may lead to
the appearance of daughter cysts in the sputum.
• If the cyst is already communicating with the bile
ducts, a bronchobiliary fistula will arise.
• Expectoration of bile-tinged sputum is a sign of
bronchobiliary fistula.
• The incidence of diaphragmatic or
transdiaphragmatic thoracic involvement by HCs in
the dome of the liver ranges from 0.6% to 16%.
57.
Communicant Rupture
• HCscan rupture into physiologic channels
(e.g., biliary, blood vessels) or adjacent organs
(e.g., digestive tract).
• In silentrupture, bile leaks from eroded small
ducts into the cyst, causing endogenic
vesiculation, suppuration, and eventually
death of the parasite. Such cysts are filled with
bile-stained detritus, although no visible bile
duct communications can be seen. Probably
80% to 90% of HC bile duct ruptures are of the
silent type.
60.
• A triadof symptoms characterizes
“symptomatic” rupture into the bile ducts:
– (a) biliary colic,
– (b) partial intermittent or complete ductal
obstruction with cholangitis and jaundice,
– (c) germinative membranes in the feces
61.
• Rupture intoa large bile duct may allow more
or less complete emptying of the fluid and
detritus and lead to spontaneous cure or
cholestatic jaundice with recurrent cholangitis.
• Incomplete emptying and a persisting
communication usually result in secondary
infection.
62.
• obstructive jaundiceare caused by intrabiliary
rupture of hepatic HCs. This type of rupture is
also called a “major communication,” has a
fistula orifice diameter of >5 mm, and
communicates with a larger bile duct. This
type of rupture is infrequent and has an
incidence of 3% to 10%.
63.
• Rupture IntoAdjacent Organ
– A HC can rupture into the digestive tract, causing
hydatidemesis or hydatidenteria.
– Rupture into the urinary tract causes hydatiduria.
– Rupture of HC into the aorta, the inferior vena
cava (VCI), the pericystic blood vessels, and the
heart with embolism.
64.
Pulmonary hydatid disease
•Lung is second commonest organ affected
after liver.
• Right lung and lower lobes are slightly more
often involved.