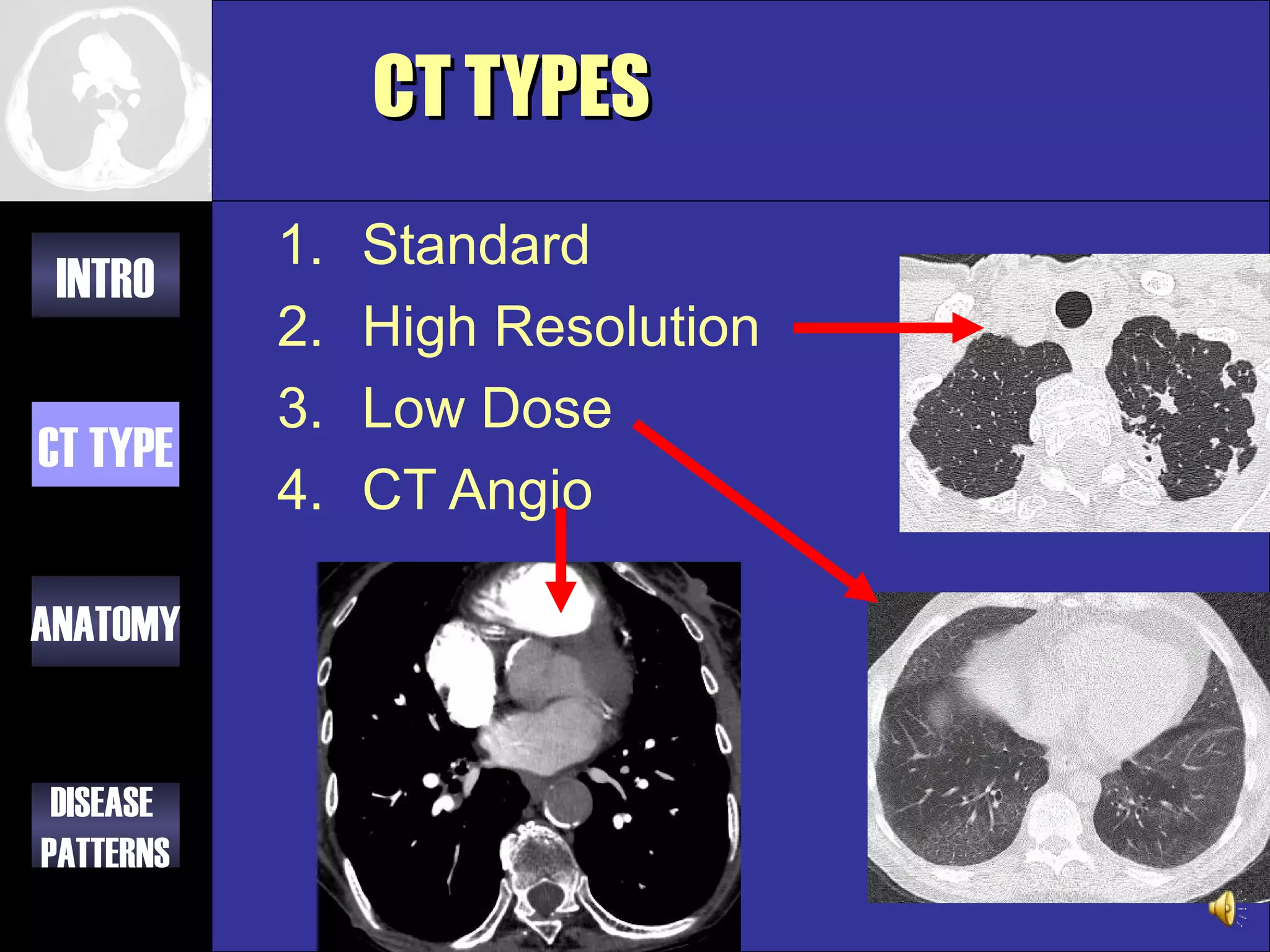
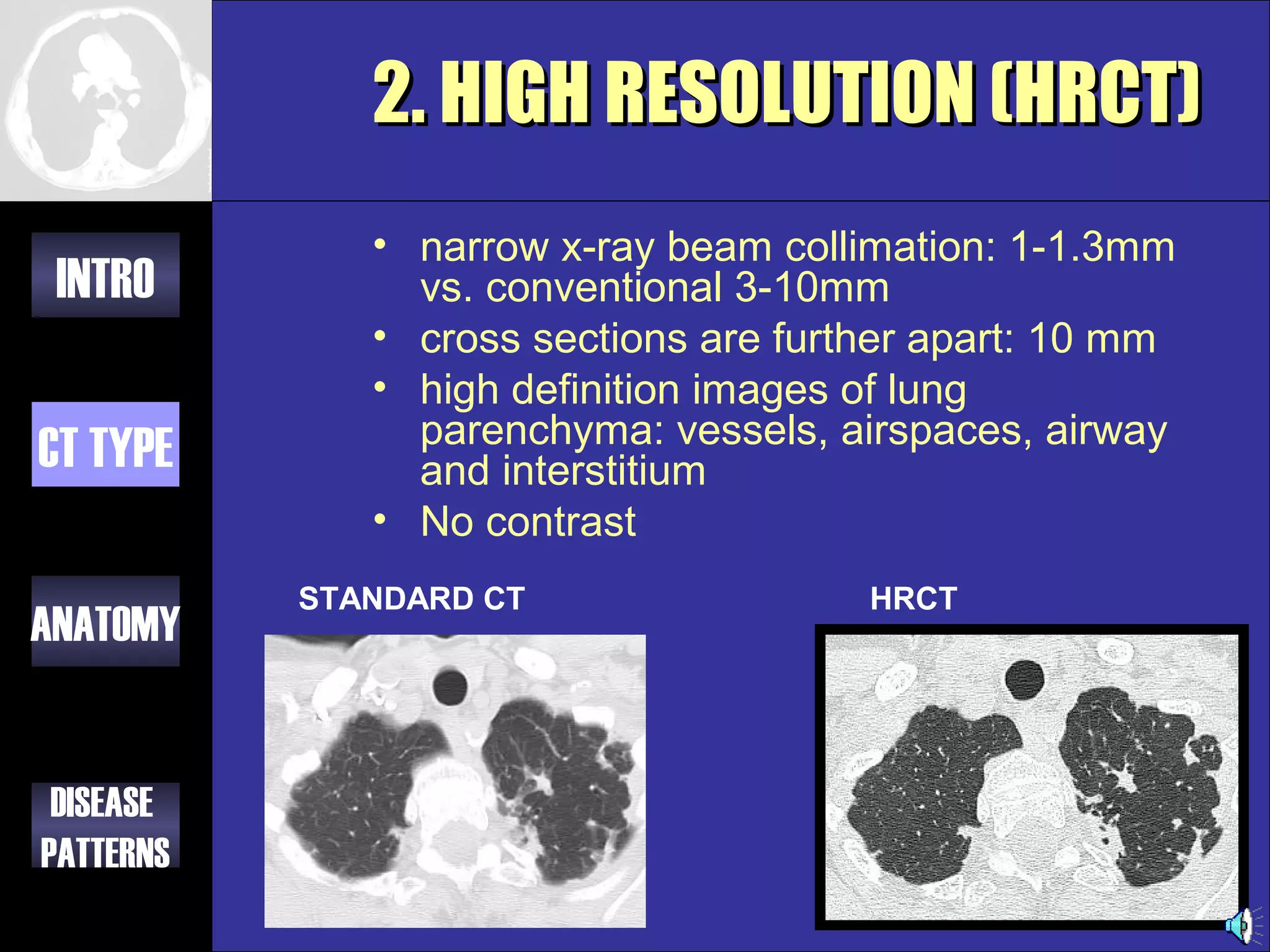
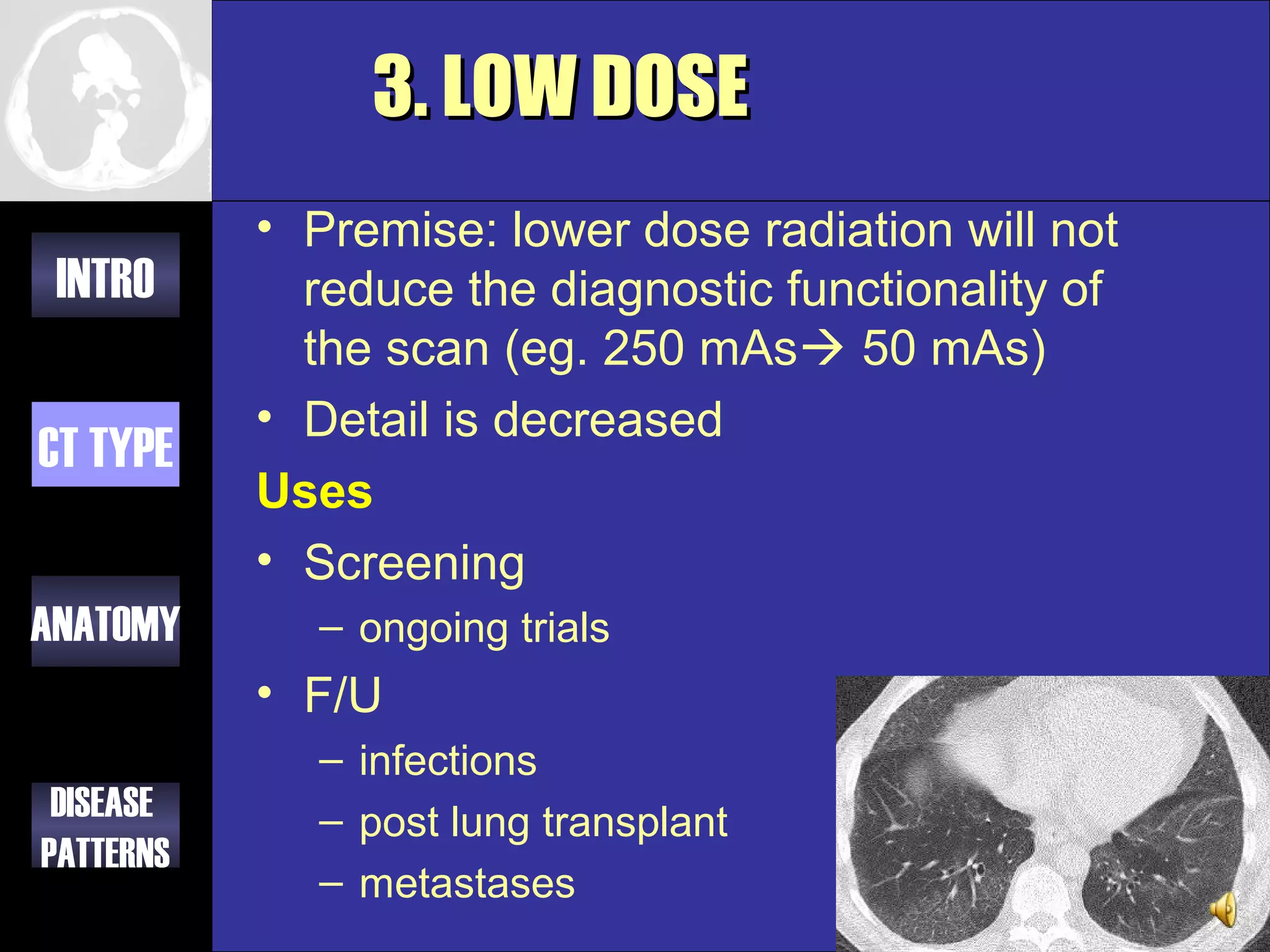
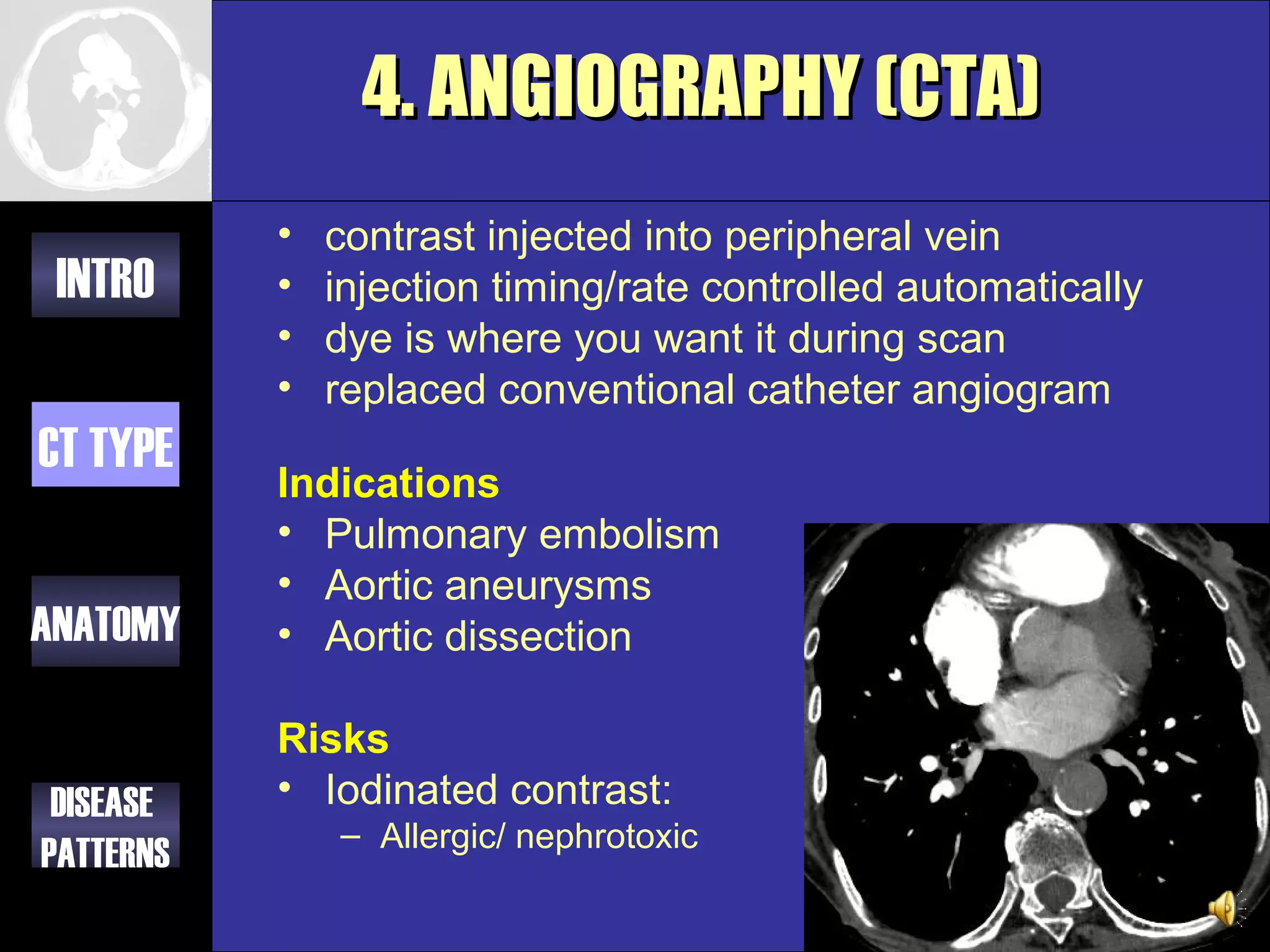
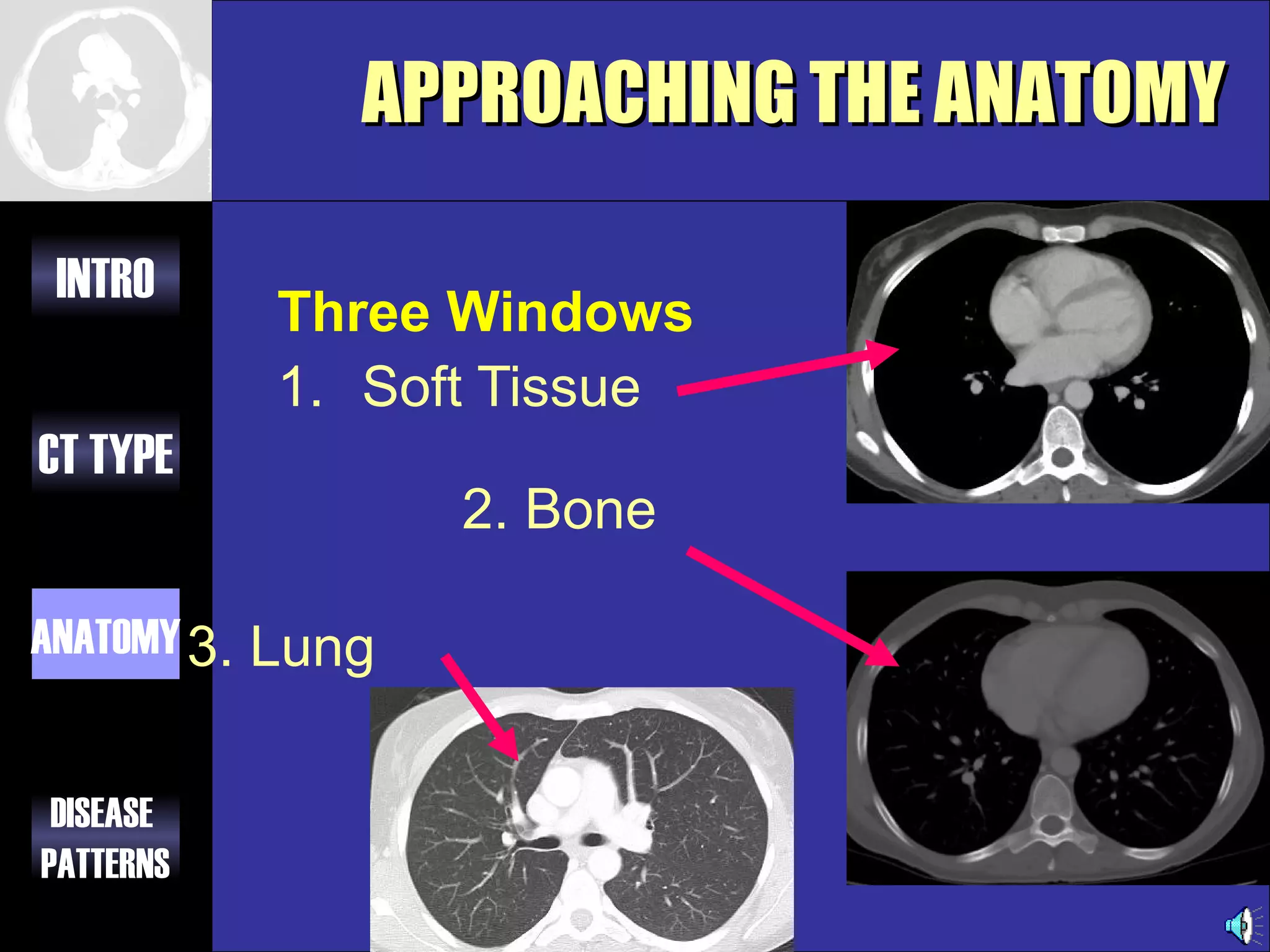
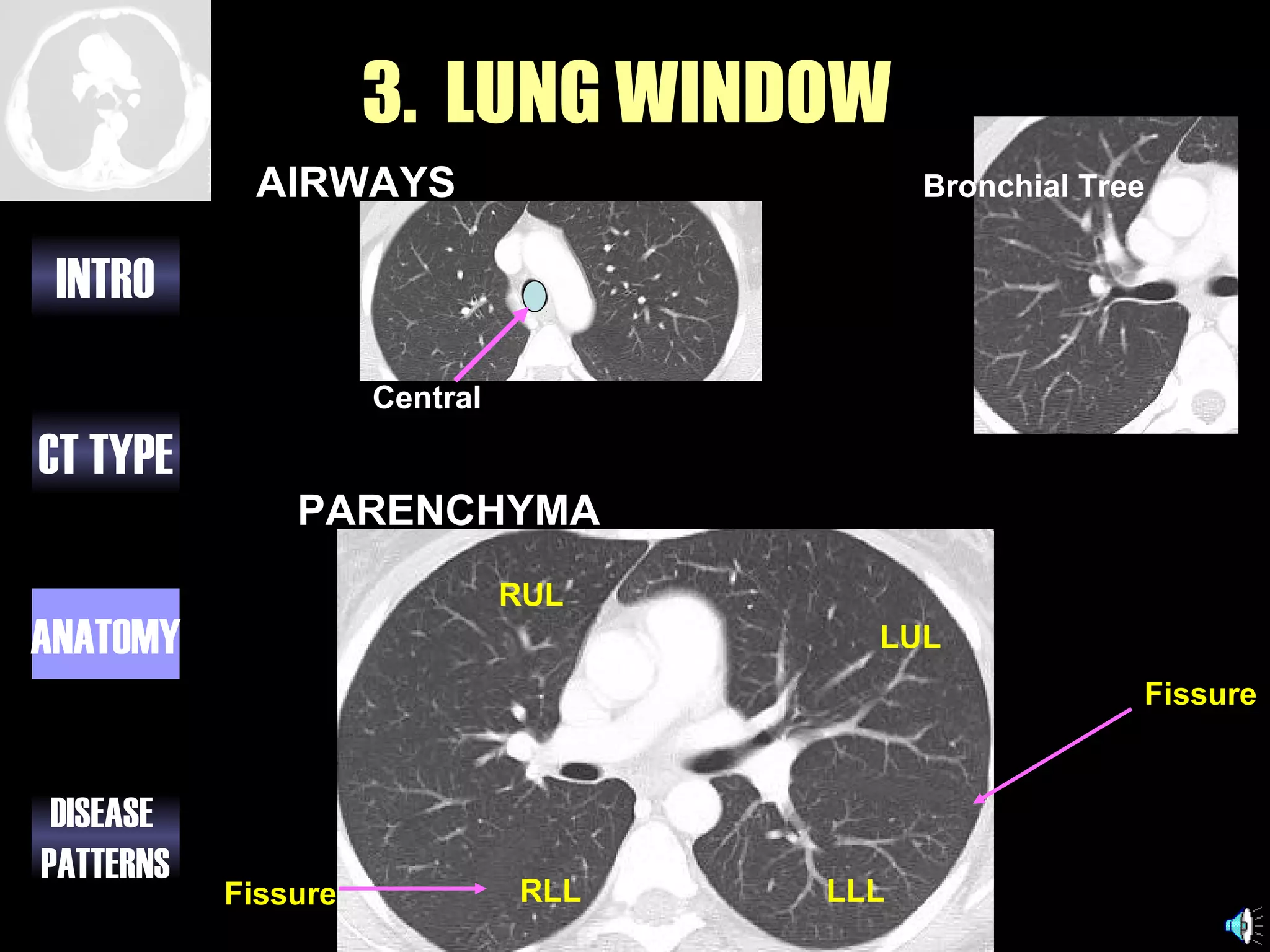
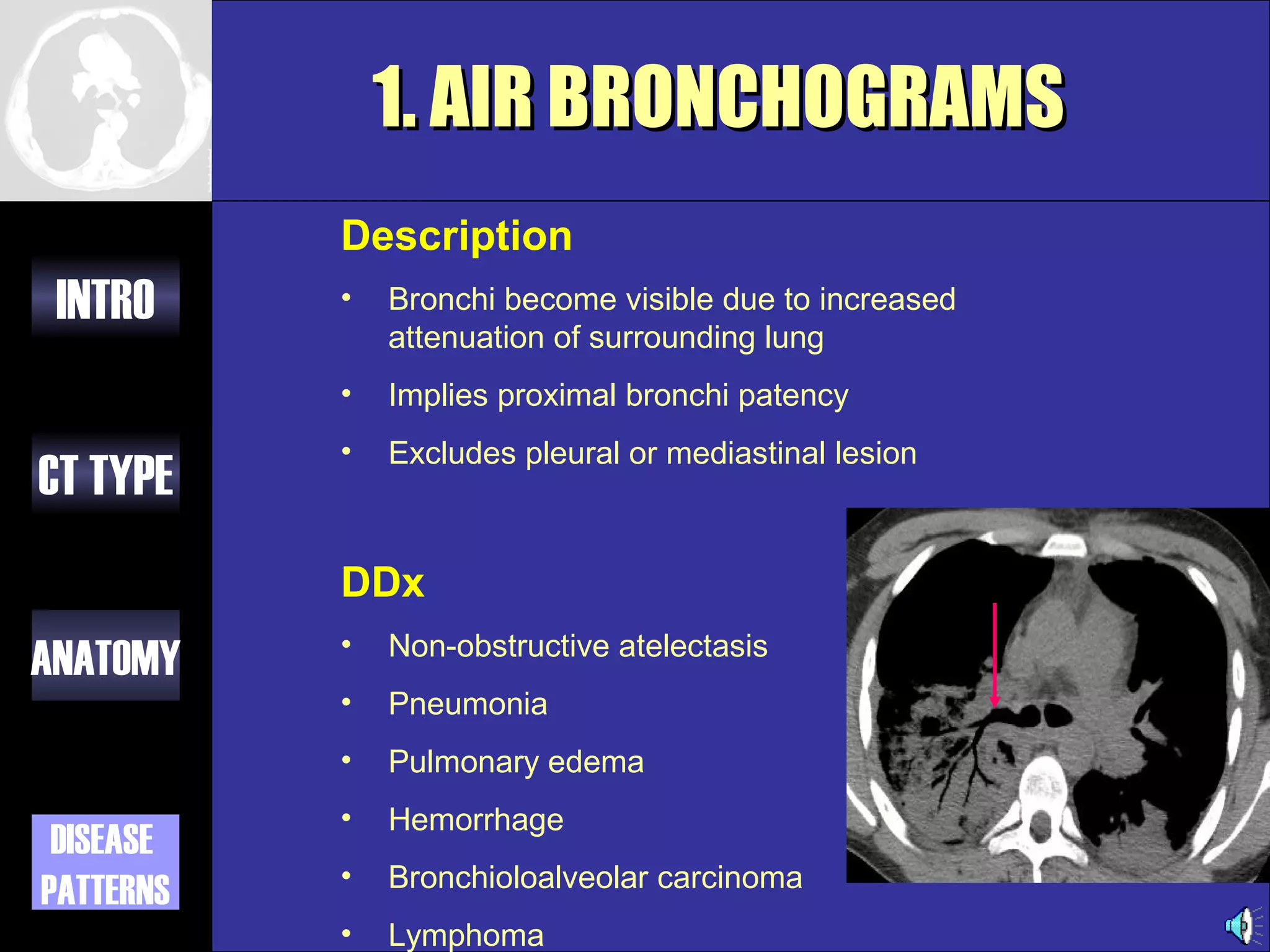
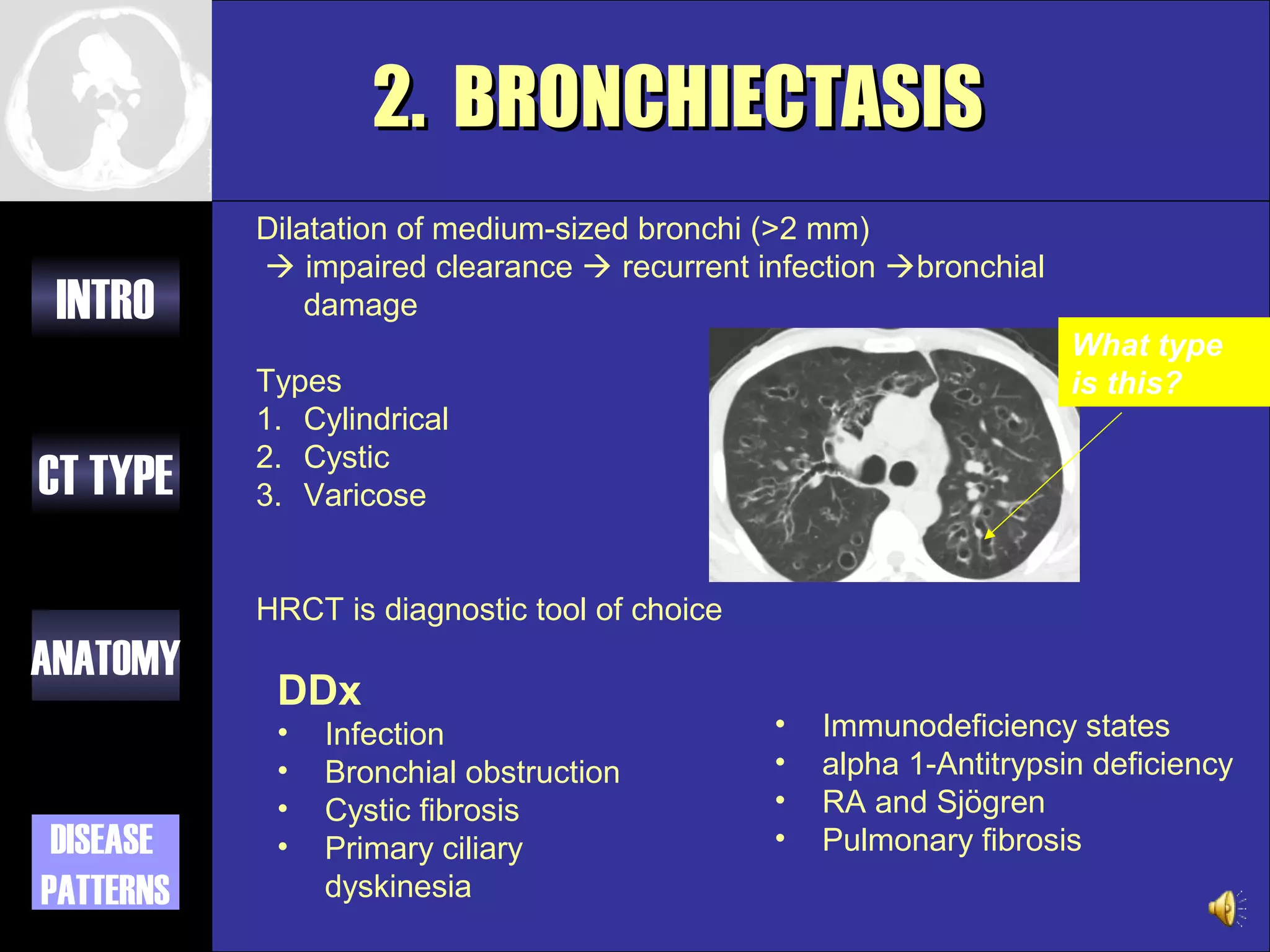
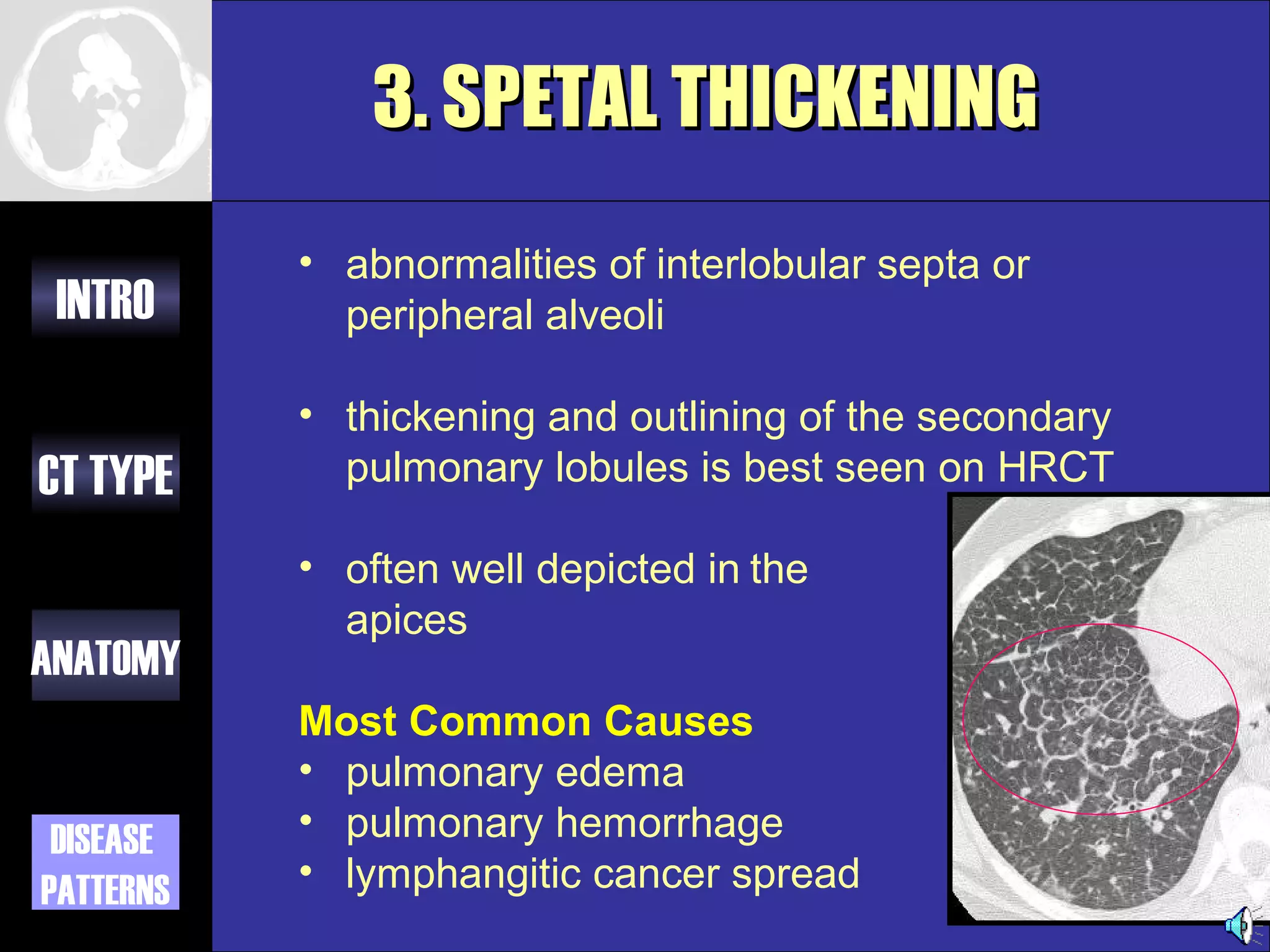
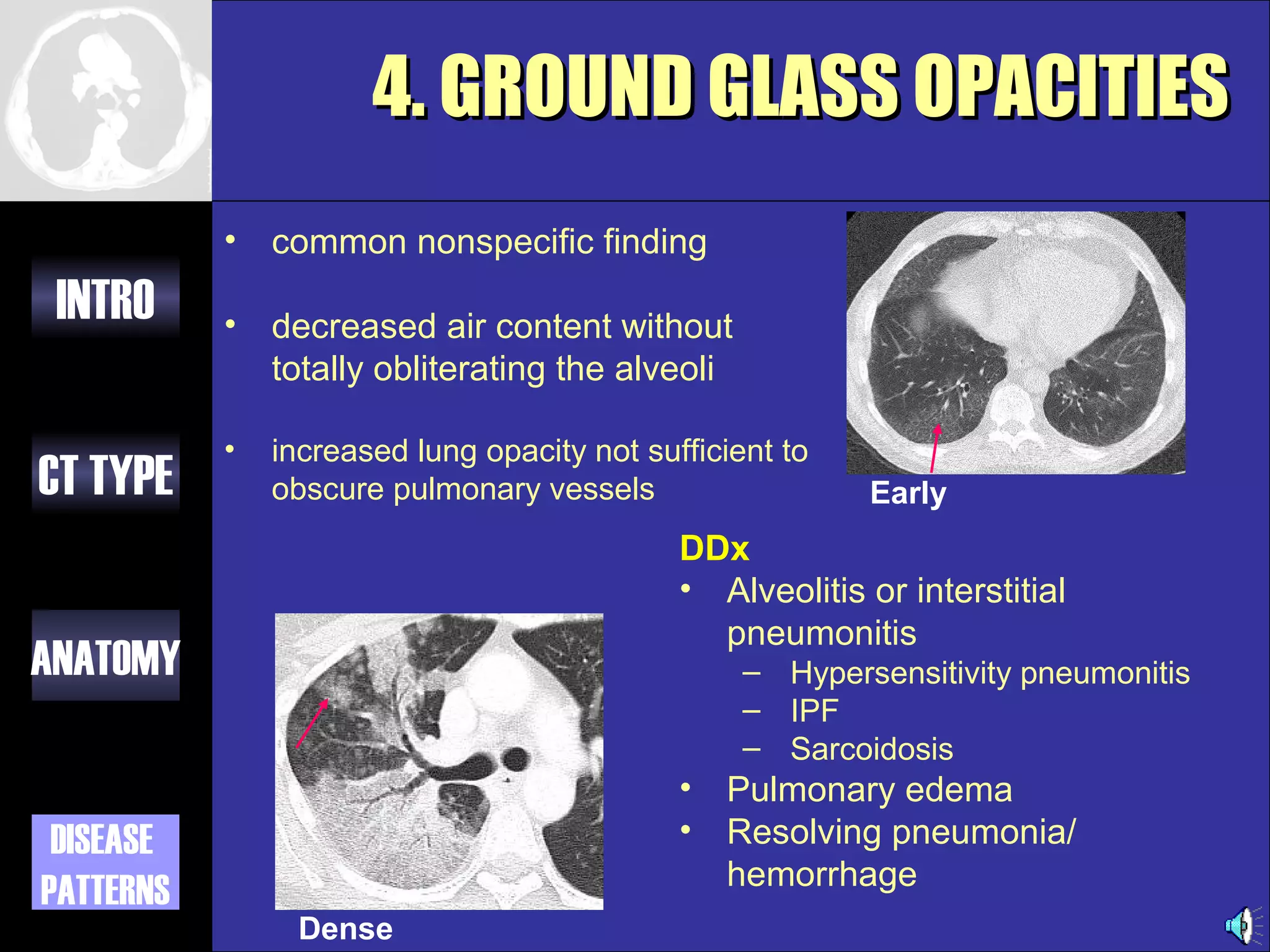
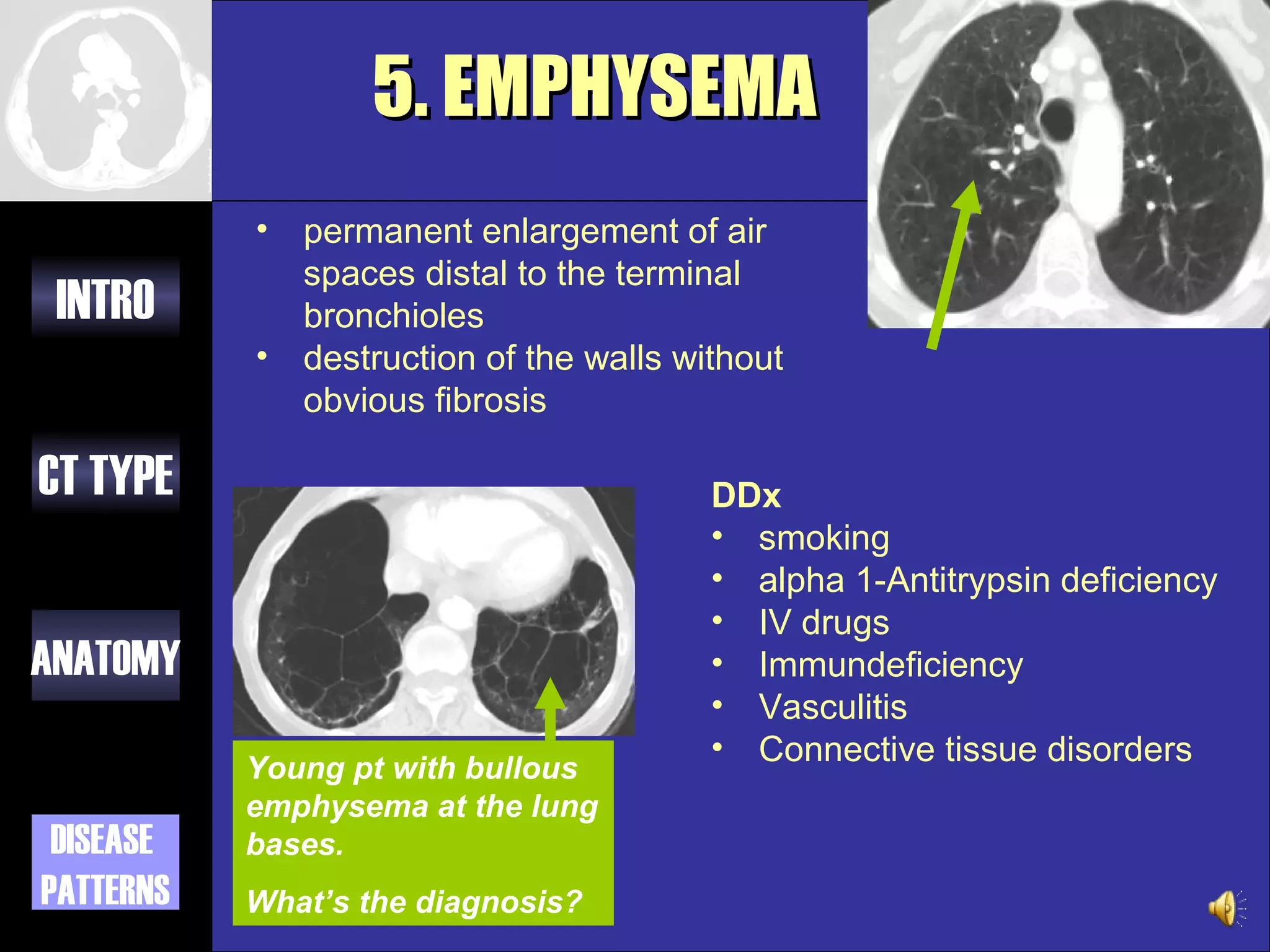
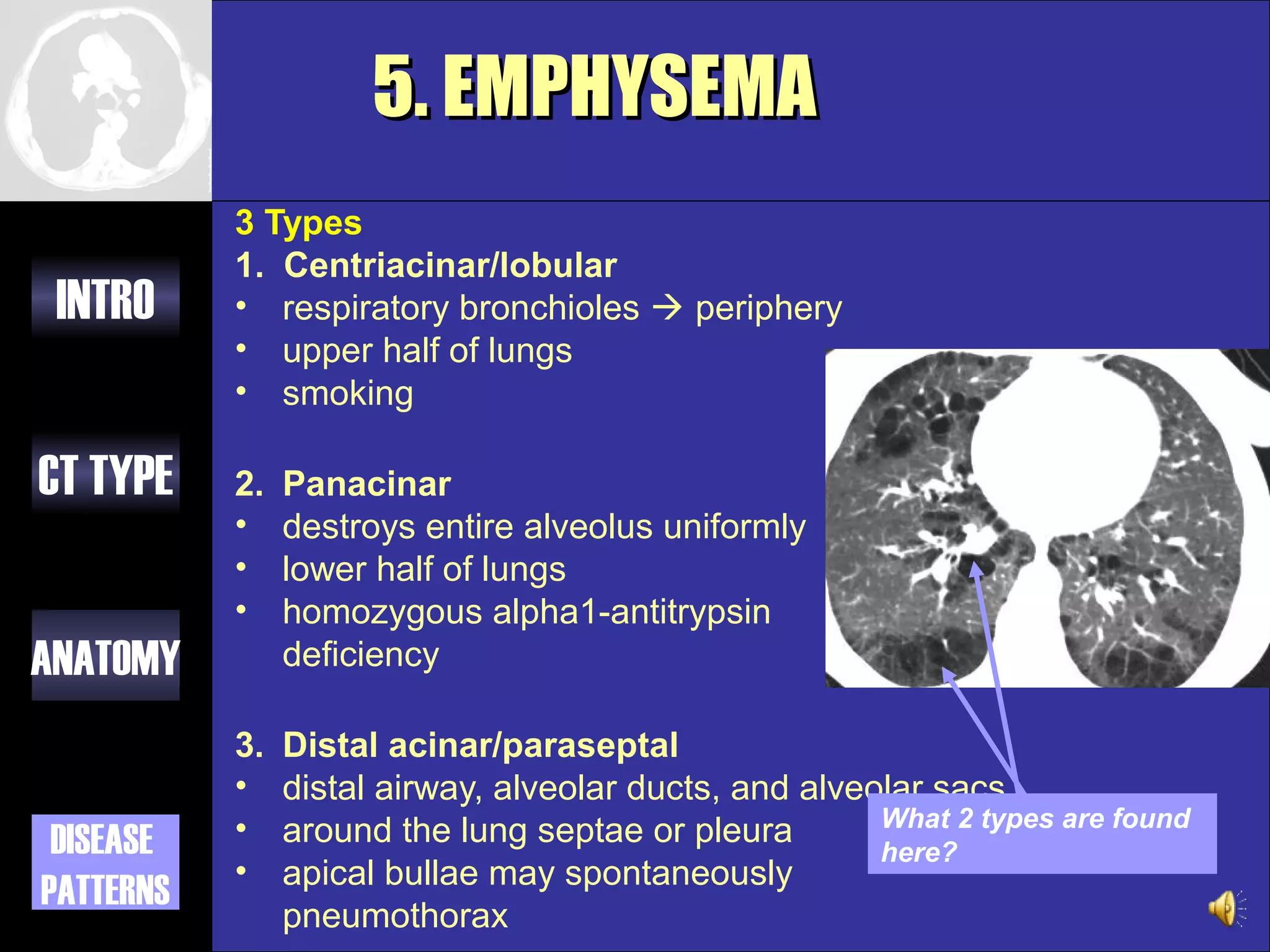
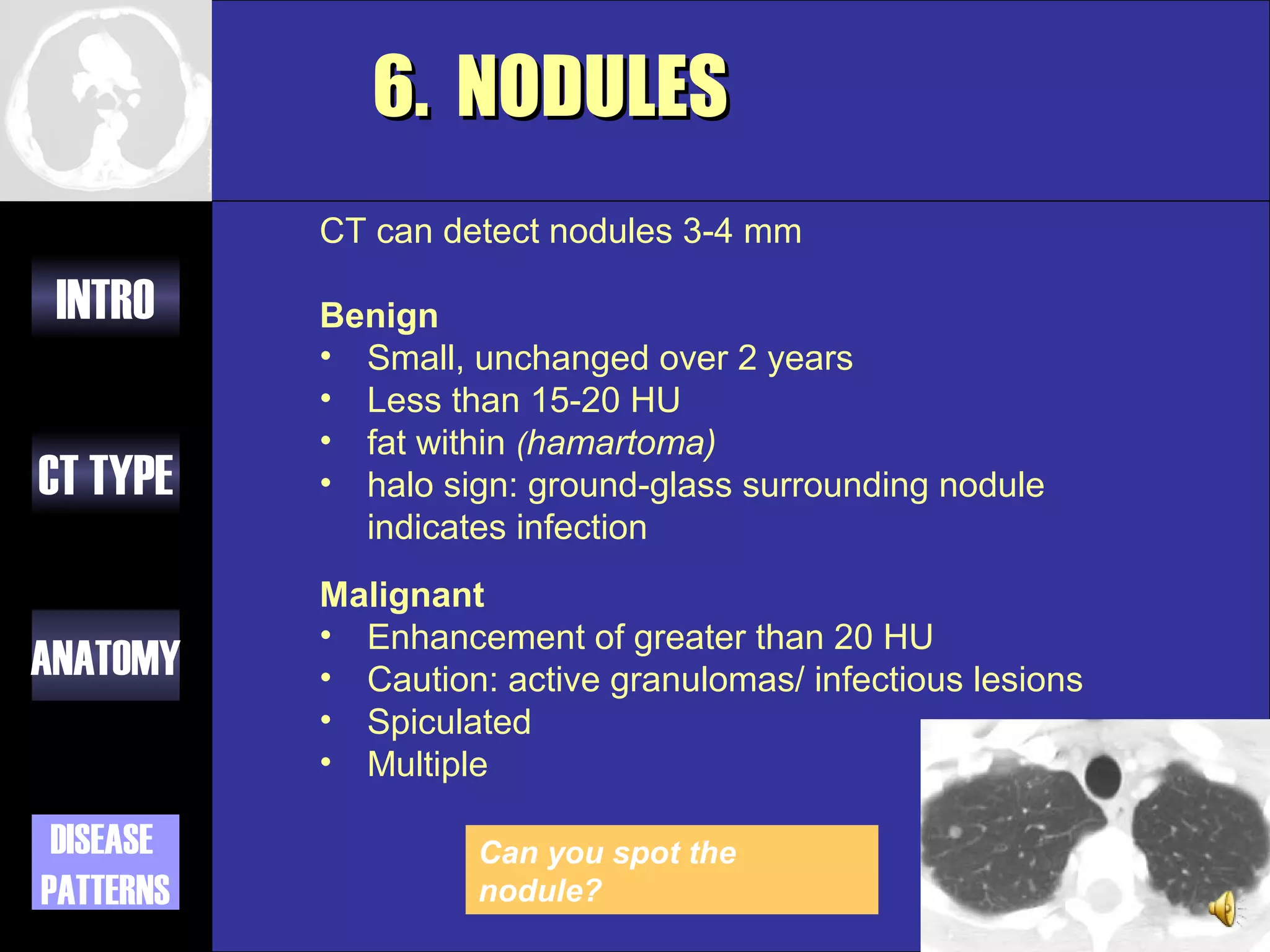
This document provides an overview of different types of CT imaging of the chest, including standard CT, high resolution CT, low dose CT, and CT angiography. It discusses the anatomy visible on chest CT scans and common disease patterns seen, such as air bronchograms, bronchiectasis, ground glass opacities, and pulmonary nodules. References are provided for further reading on CT signs of lung disease.