Downloaded 21 times
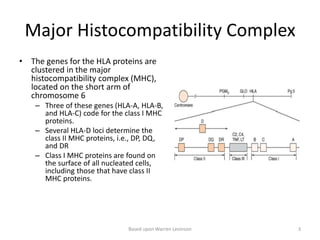
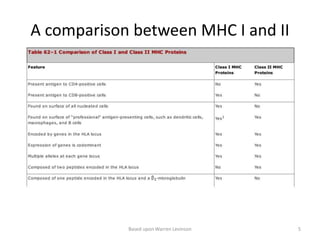

This document discusses HLA transplantation and the complement system. It begins by explaining that the success of organ transplants depends on donor and recipient HLA proteins matching. It then describes that HLA proteins are encoded by genes in the MHC located on chromosome 6, and are classified as class I or II proteins. The document provides details on MHC protein structure and expression, as well as the biological importance of MHC in antigen presentation and T cell recognition. It defines types of transplants and explains transplant rejection processes. Finally, it gives an overview of the complement system, describing its activation pathways and roles in immune responses like opsonization, chemotaxis, and cytolysis.


























































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)














