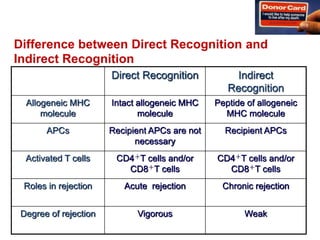
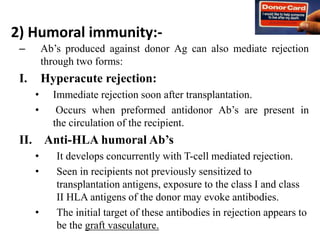
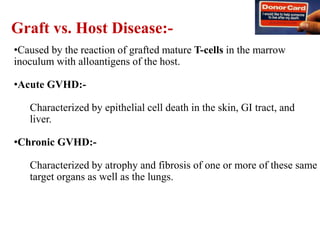
This document summarizes key information about transplantation. It discusses the definition of transplantation as the transfer of organs or tissues between parts of the body or between individuals. The most common types of transplantation are discussed, including blood transfusions and organs like the kidneys, heart, and liver. The document also describes the immune mechanisms involved in graft rejection, such as cell-mediated and humoral immunity. It provides details on the different types of graft rejection and classifications of transplantation based on genetic differences between donors and recipients.






































![19 chronic%20 gvhd[1]](https://cdn.slidesharecdn.com/ss_thumbnails/19chronic20gvhd1-120910150049-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


















































