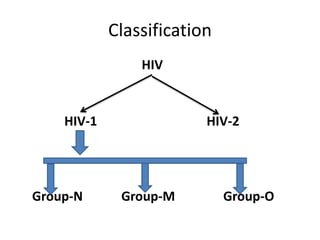
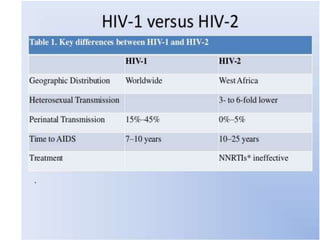
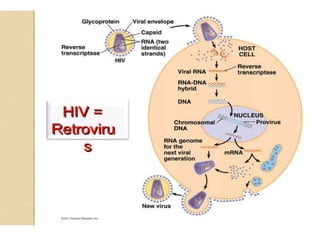
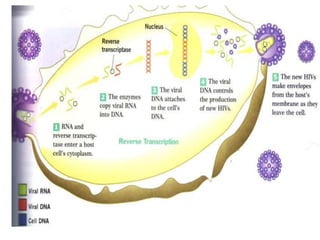
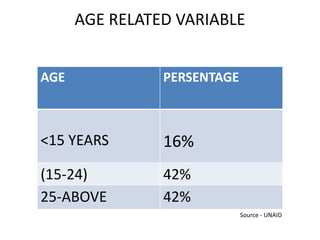
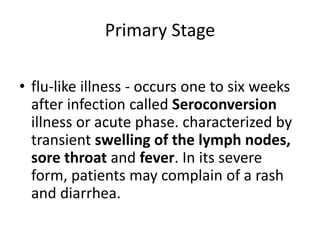
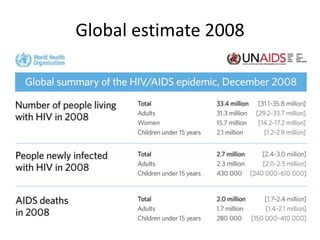
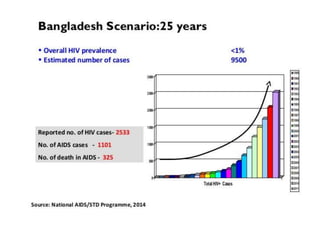
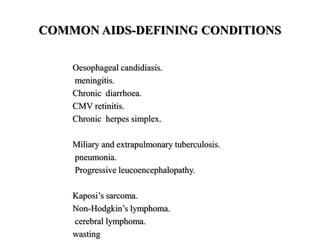
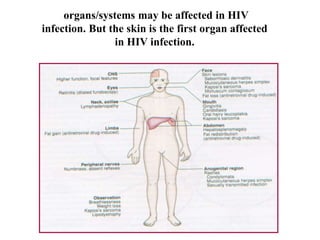
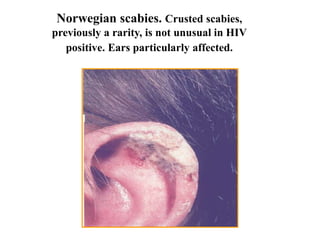
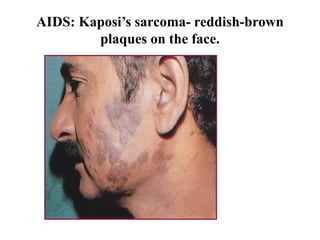
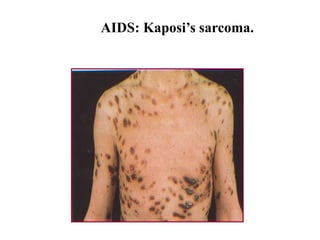
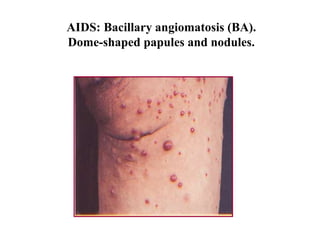
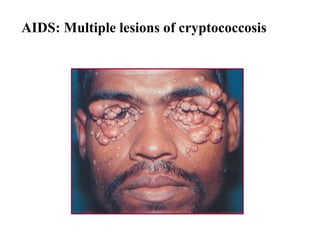
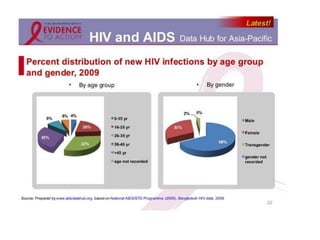
This document provides a summary of the history and epidemiology of HIV/AIDS. It discusses the initial cases reported in 1979 and the evolving understanding and naming of the virus. Key points include: HIV is classified into two types, HIV-1 being more easily transmitted than HIV-2; it is transmitted via bodily fluids and progresses from primary infection to asymptomatic infection to symptomatic AIDS if untreated; common opportunistic infections associated with AIDS are also outlined. The document then focuses on the epidemiology of HIV/AIDS globally and nationally in Bangladesh.


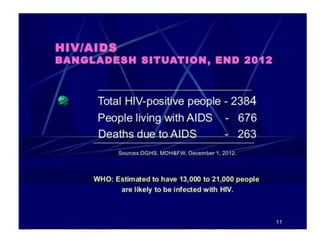





![HIV and AIDS estimates IN BANGLADESH (2014)
Number of people living with HIV 8,900 [8,000 - 9,800]
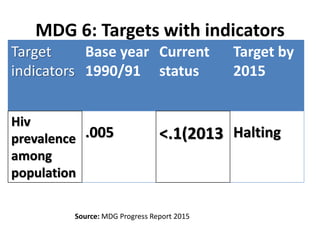
Adults aged 15 to 49 prevalence rate <0.1% [<0.1% - <0.1%]
Adults aged 15 and up living with HIV 8,600 [7,700 - 9,400]
Women aged 15 and up living with HIV 2,900 [2,600 - 3,100]
Children aged 0 to 14 living with HIV <500 [<500 - <500]
Deaths due to AIDS <1000 [<1000 - 1,200]
Orphans due to AIDS aged 0 to 17 N/A](https://image.slidesharecdn.com/hivpresentation-160229092036/85/HIV-and-AIDS-66-320.jpg)
































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

