Downloaded 19 times


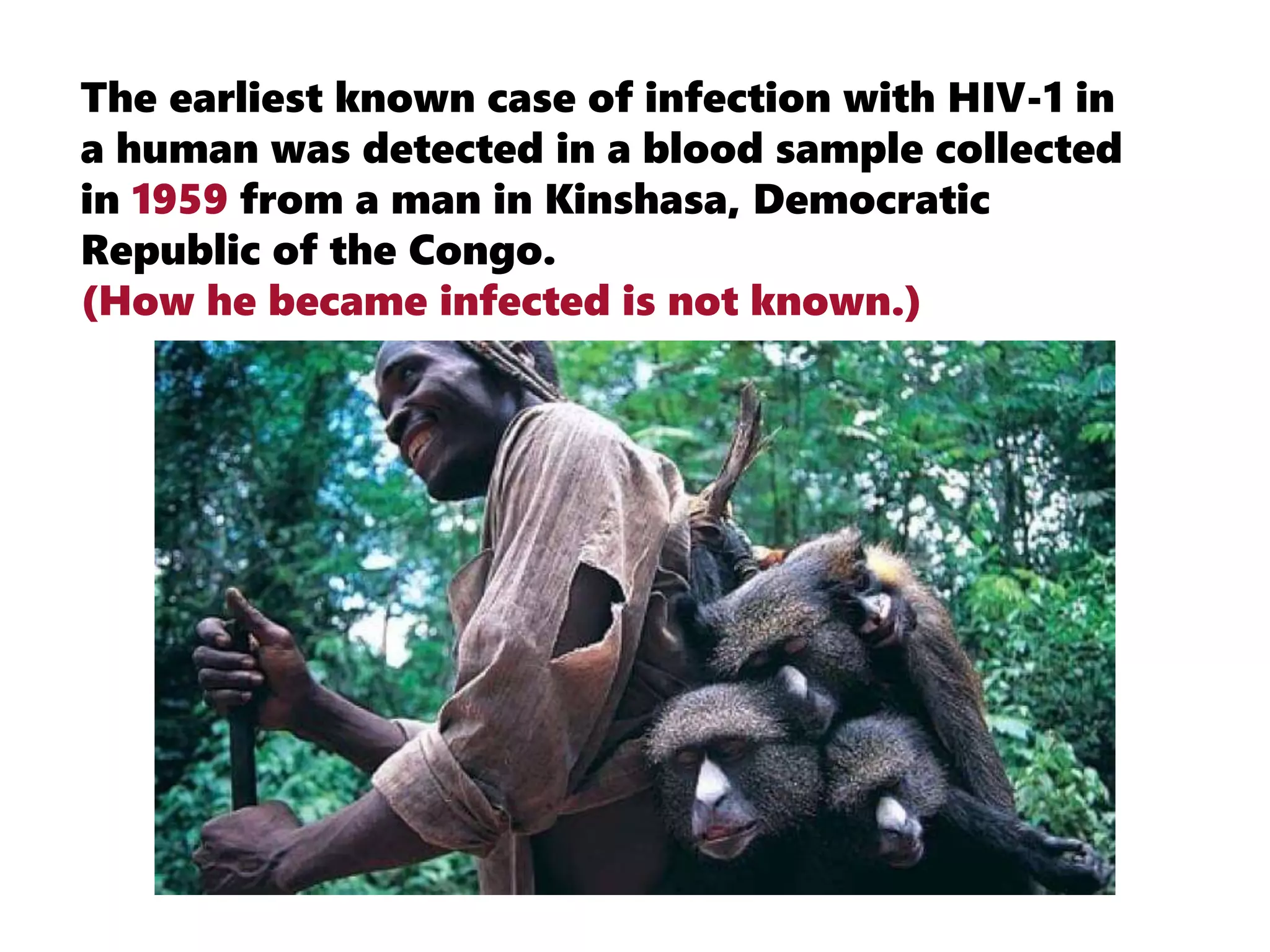





















































































































HIV originated from chimpanzees in West Africa and was transmitted to humans. The earliest known case of HIV in a human was detected in 1959 in the Democratic Republic of Congo. Antiretroviral therapy uses HIV medicines to treat infection and suppress viral load, preventing transmission. Factors like viral load, condom use, and adherence to medication determine likelihood of HIV transmission. Common signs of HIV infection include fever, fatigue, swollen lymph nodes, and skin rashes.



































































