Downloaded 15 times









































![ARV REGIMENS
• First Line ARV regimens
-{ AZT/3TC + NVP or EFV ] Recommended
- TDF/FTC + NVP or EFV
• Women of Childbearing age who may get pregnant
• AZT/3TC + NVP or
• TDF/FTC + NVP
•
• Any patients with TB co infection
• AZT/3TC + EFV or
• TDF/FTC + EFV](https://image.slidesharecdn.com/hiv-150203200308-conversion-gate02/85/Hiv-68-320.jpg)







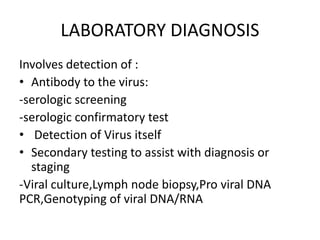
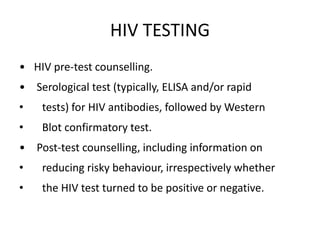
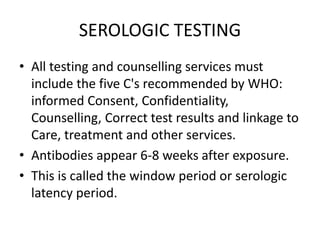
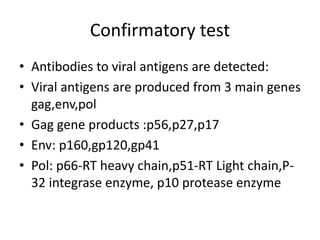
The document provides an extensive overview of Human Immunodeficiency Virus (HIV), including its types, transmission methods, epidemiology, and clinical features. It discusses the immunopathophysiology of HIV, the progression of the infection, the impact on various immune cells, and opportunistic infections and cancers associated with AIDS. Additionally, it details the laboratory diagnosis, treatment recommendations, and the classifications used to stage the disease.


























































![HUMAN_IMMUNODEFICIENCY_VIRUS[1]. pptx](https://cdn.slidesharecdn.com/ss_thumbnails/humanimmunodeficiencyvirus1-250922103632-2012e6ee-thumbnail.jpg?width=640&height=640&fit=bounds)




























