Downloaded 361 times


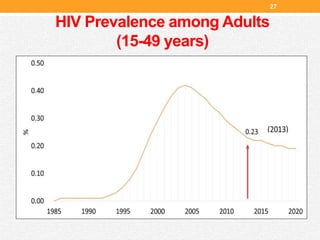
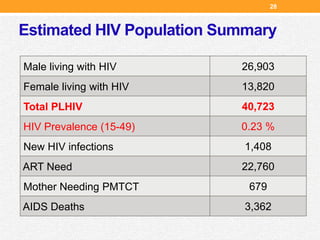
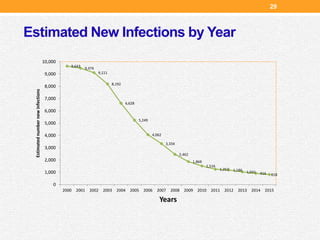



The document is an orientation presentation by Sagun Paudel outlining HIV, AIDS, and STIs, focusing on knowledge development for prevention and treatment in Nepal. It covers the transmission modes, clinical features, risk populations, and prevention strategies, as well as the history of HIV in Nepal since its first reported cases in 1988. Key statistics on HIV prevalence and the importance of voluntary counseling and testing are also included.






















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)