Downloaded 166 times
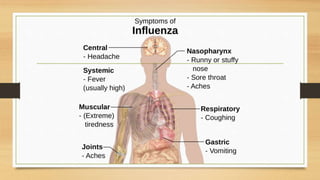



Influenza is a highly contagious viral infection that causes fever, body aches, and respiratory symptoms. It spreads easily and can cause severe illness especially in young children, elderly adults, and those with weakened immune systems. The influenza virus is classified into types A, B, and C. Type A causes the most serious disease. Symptoms are diagnosed through viral testing of respiratory samples. Complications can include pneumonia, which is especially dangerous for high-risk groups. Treatment focuses on antiviral drugs that target the virus's neuraminidase or M2 proteins.









































































