Downloaded 1,153 times

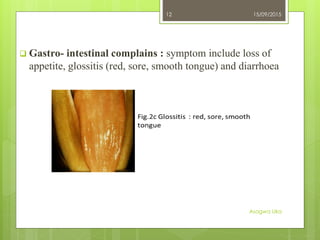
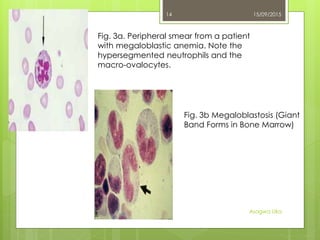
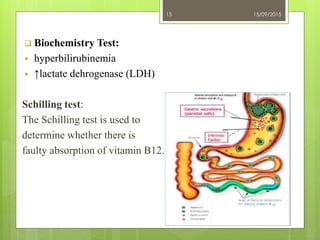
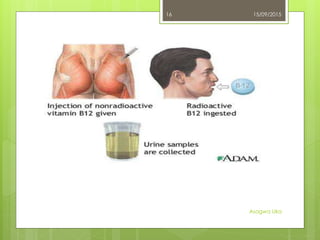


Megaloblastic anemia is a red blood cell disorder caused by inhibited DNA synthesis, mainly due to vitamin B12 or folic acid deficiencies. Symptoms include anemia, neurological issues, and gastrointestinal complaints, while laboratory diagnosis indicates various changes in blood counts and bone marrow. Treatment involves addressing nutritional deficiencies by targeting sources rich in vitamin B12 and folic acid.

































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
