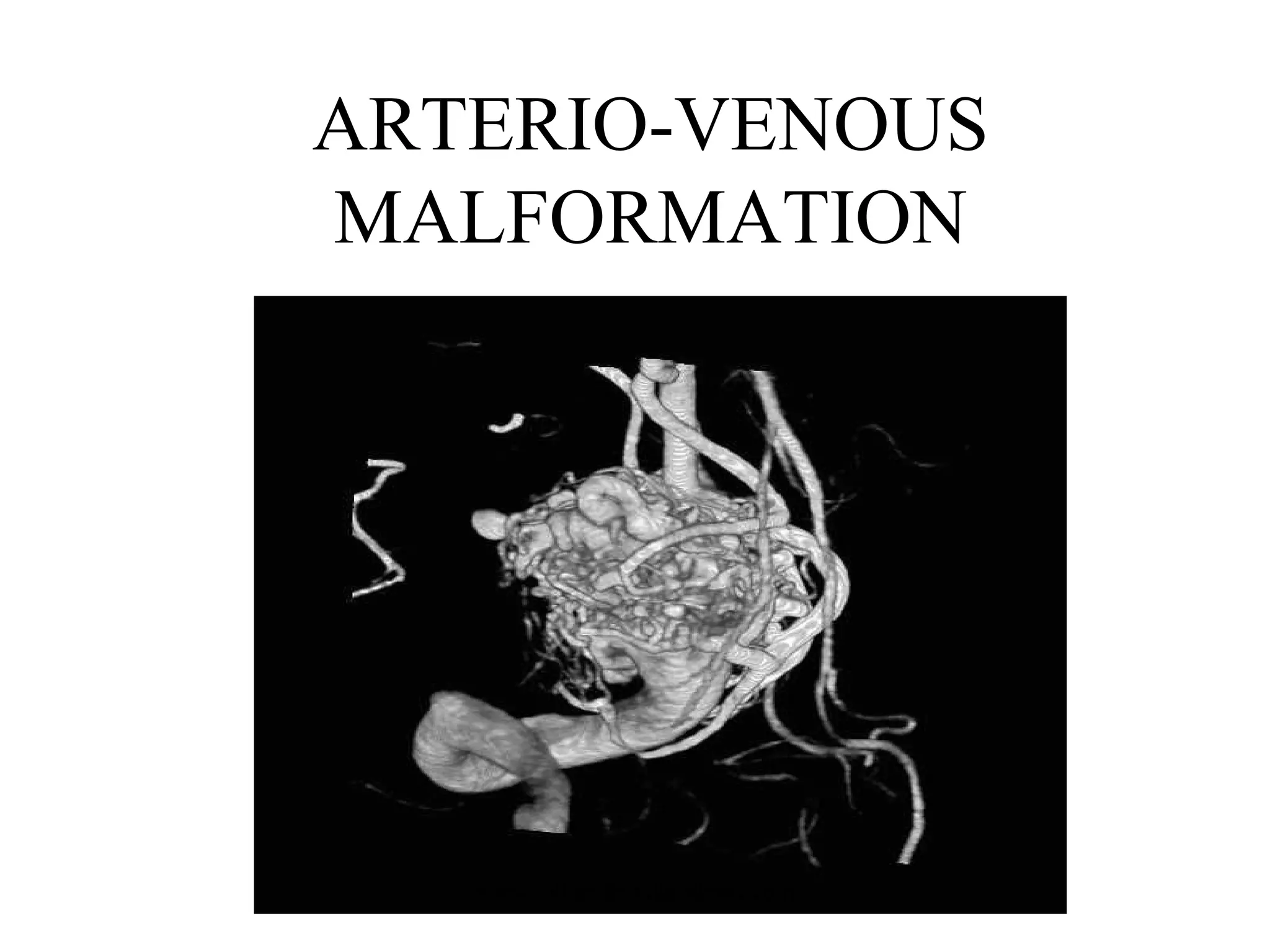
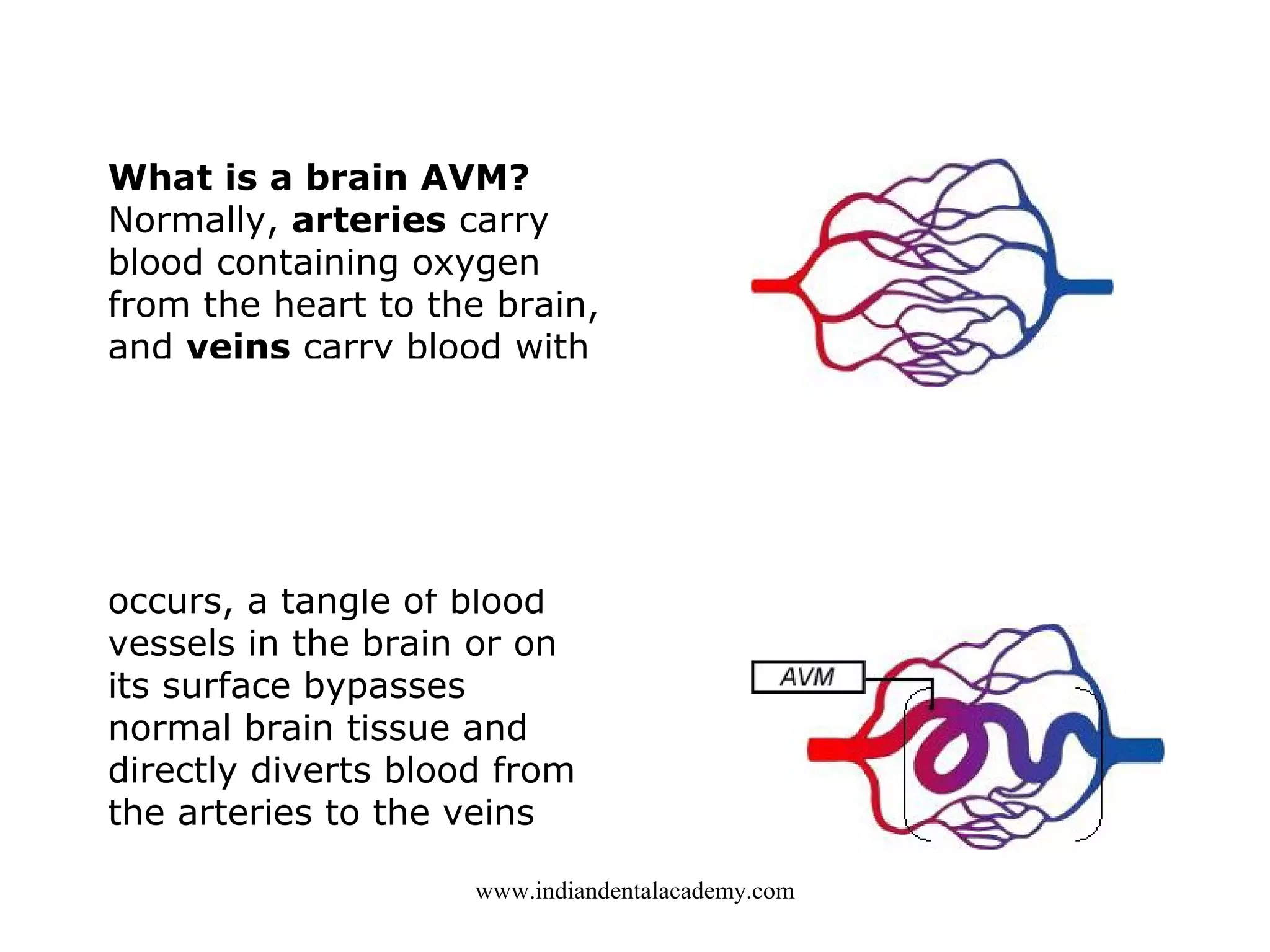
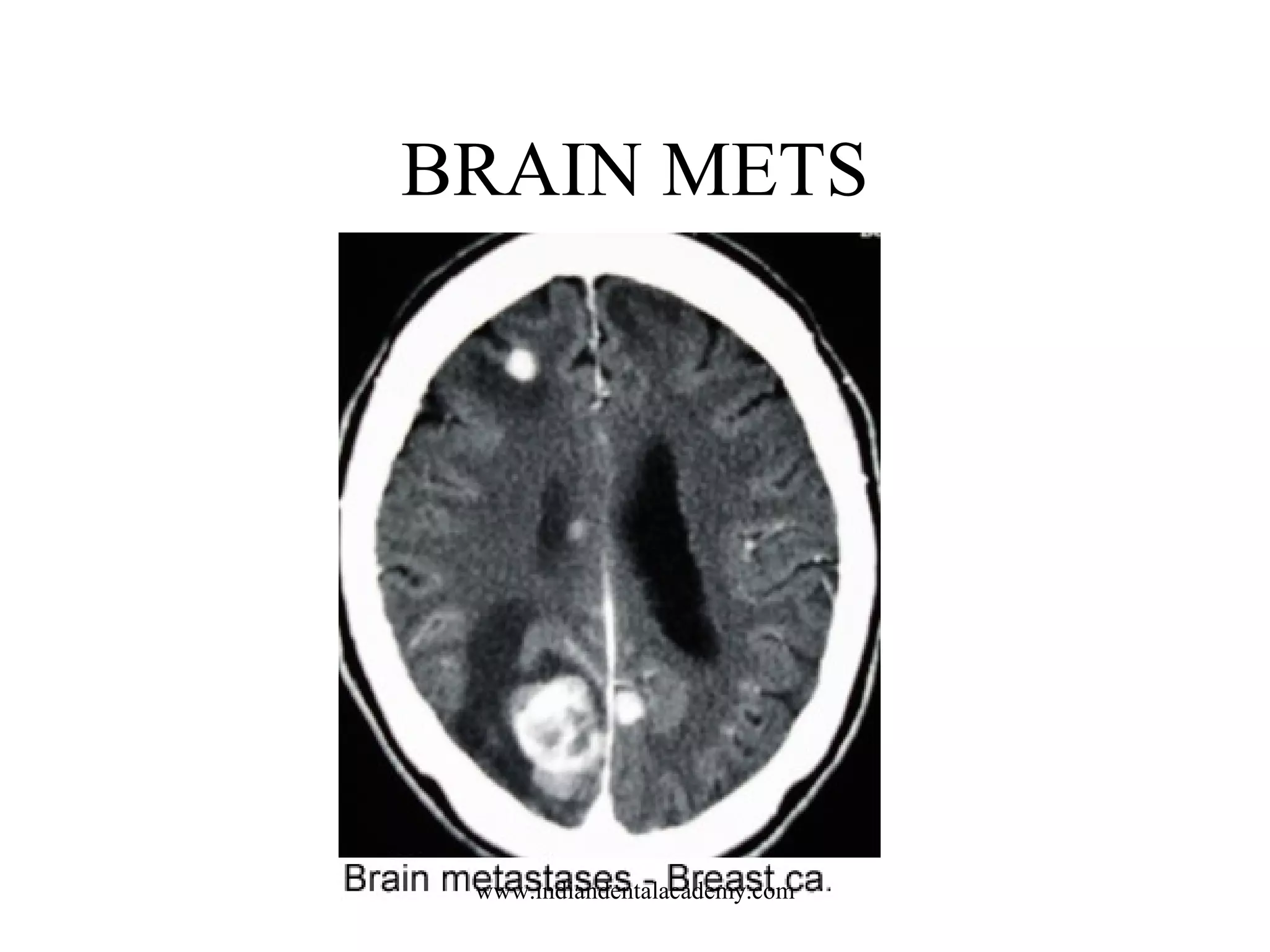
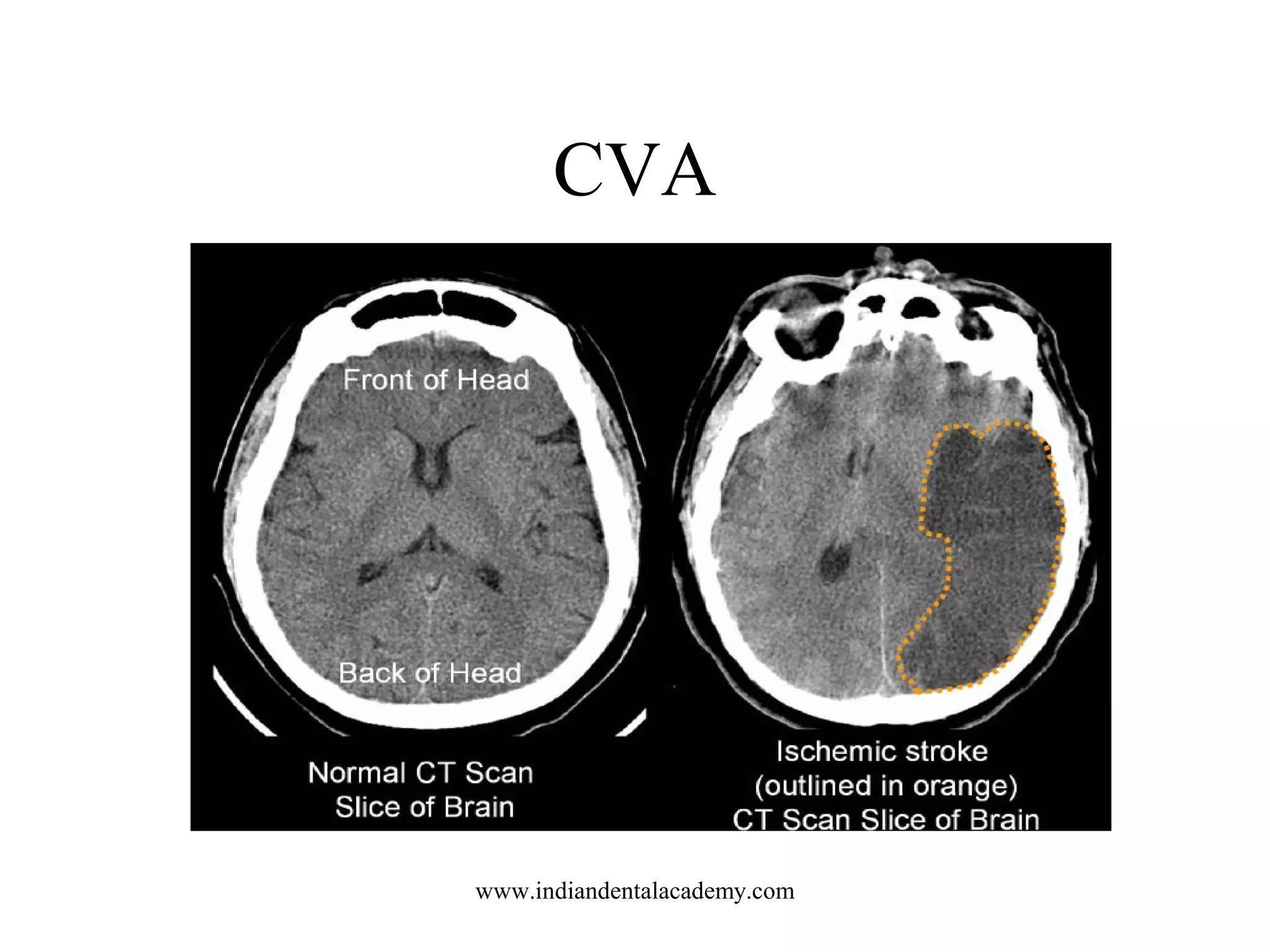
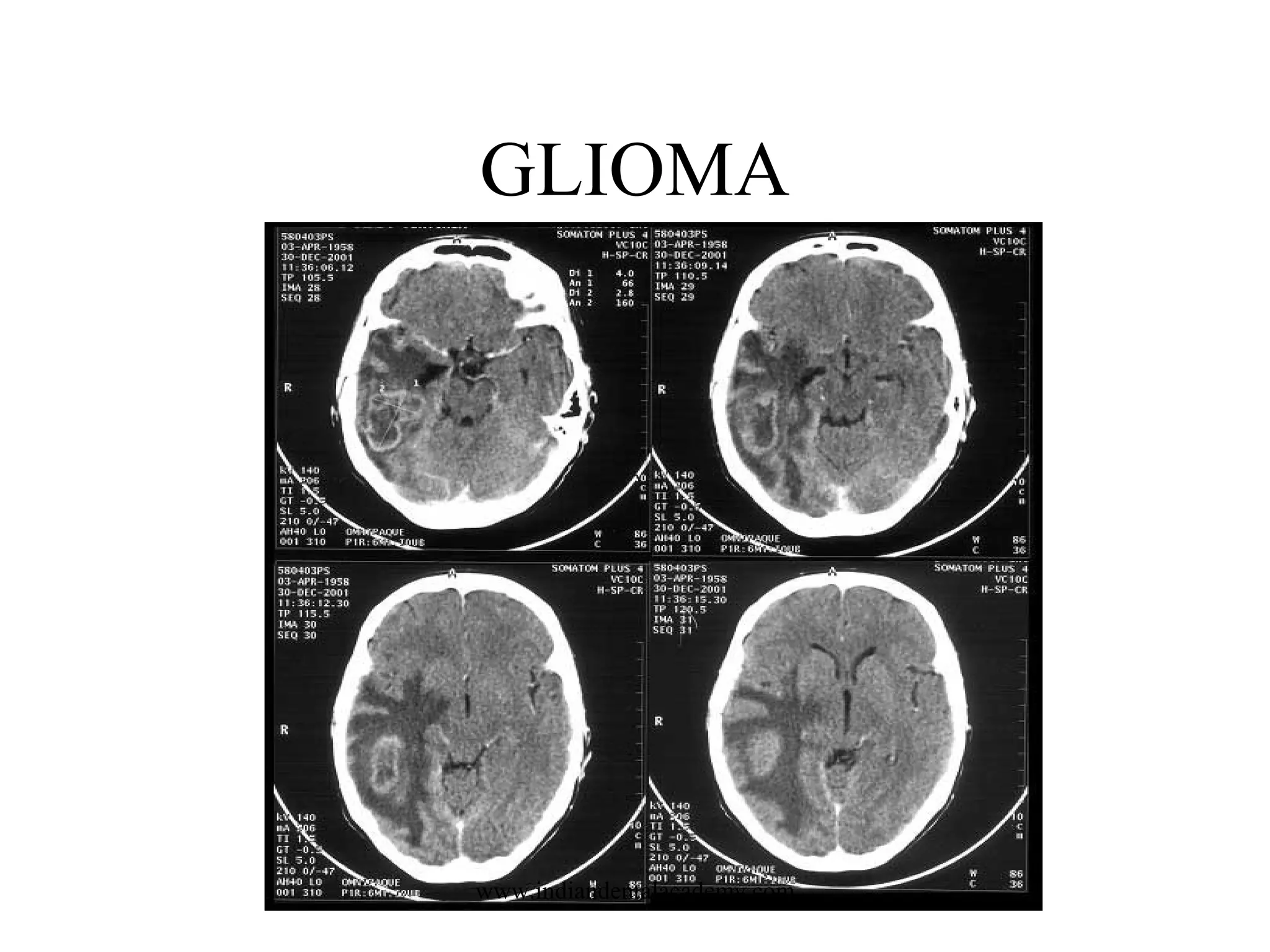
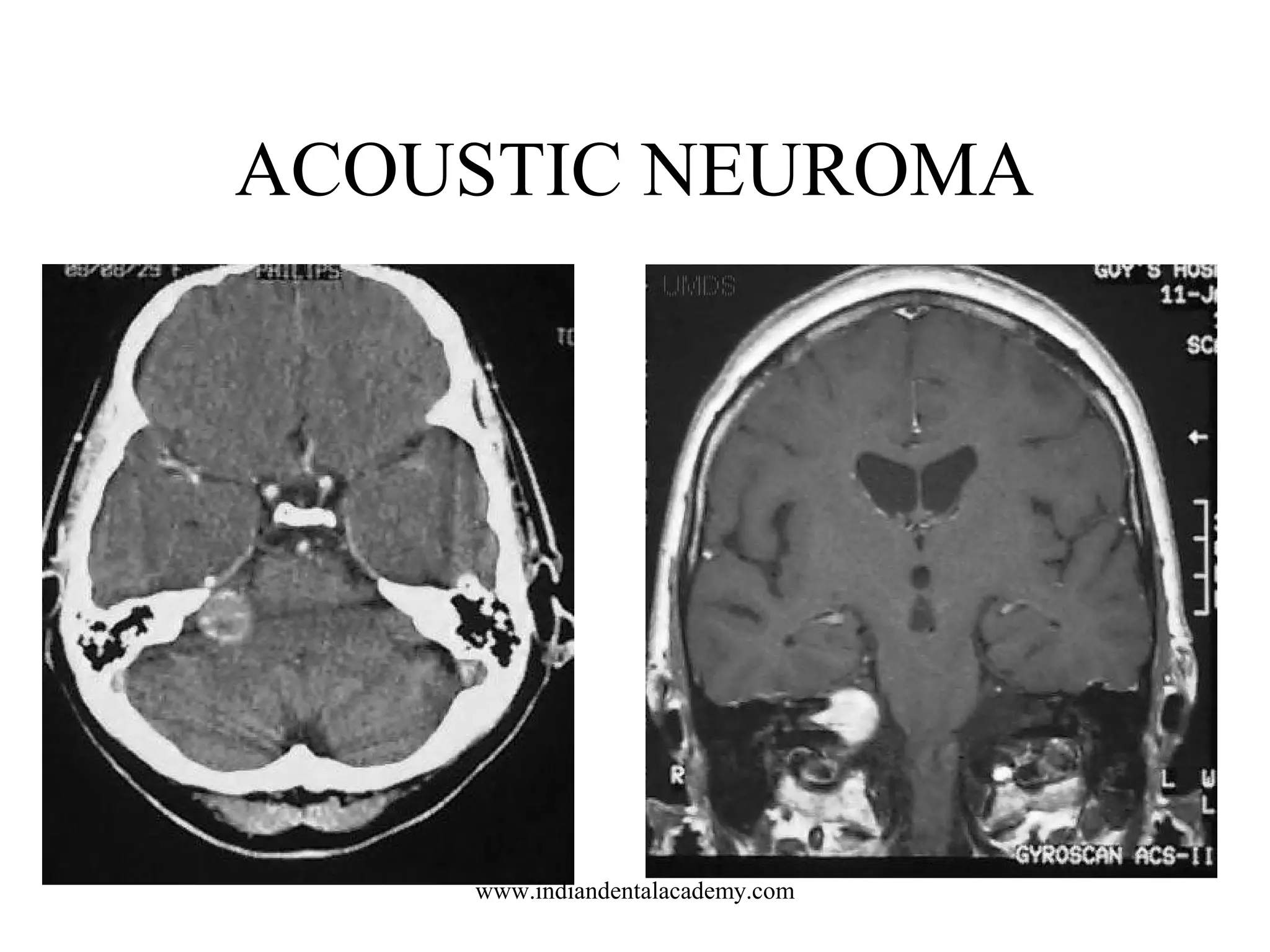
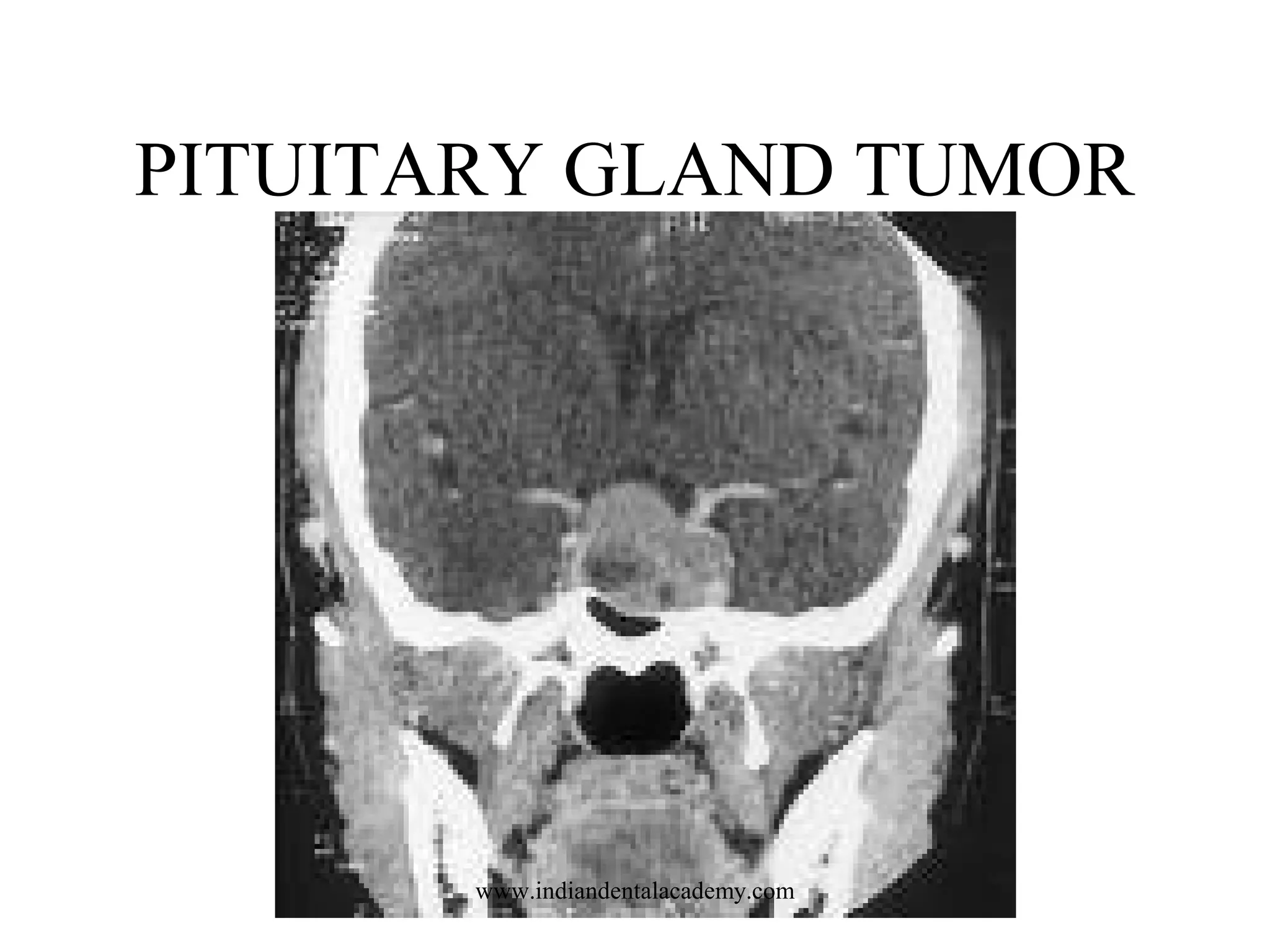

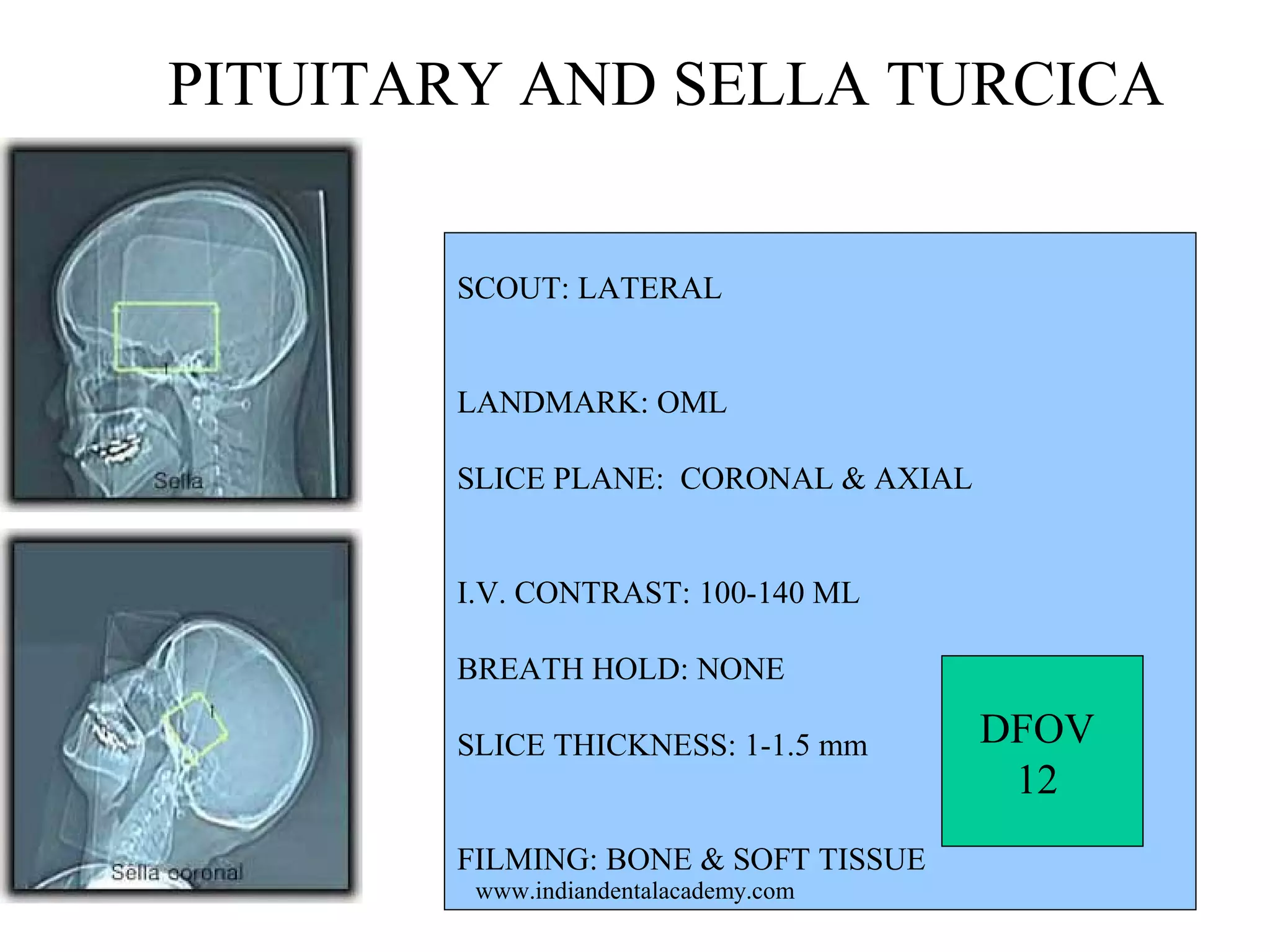


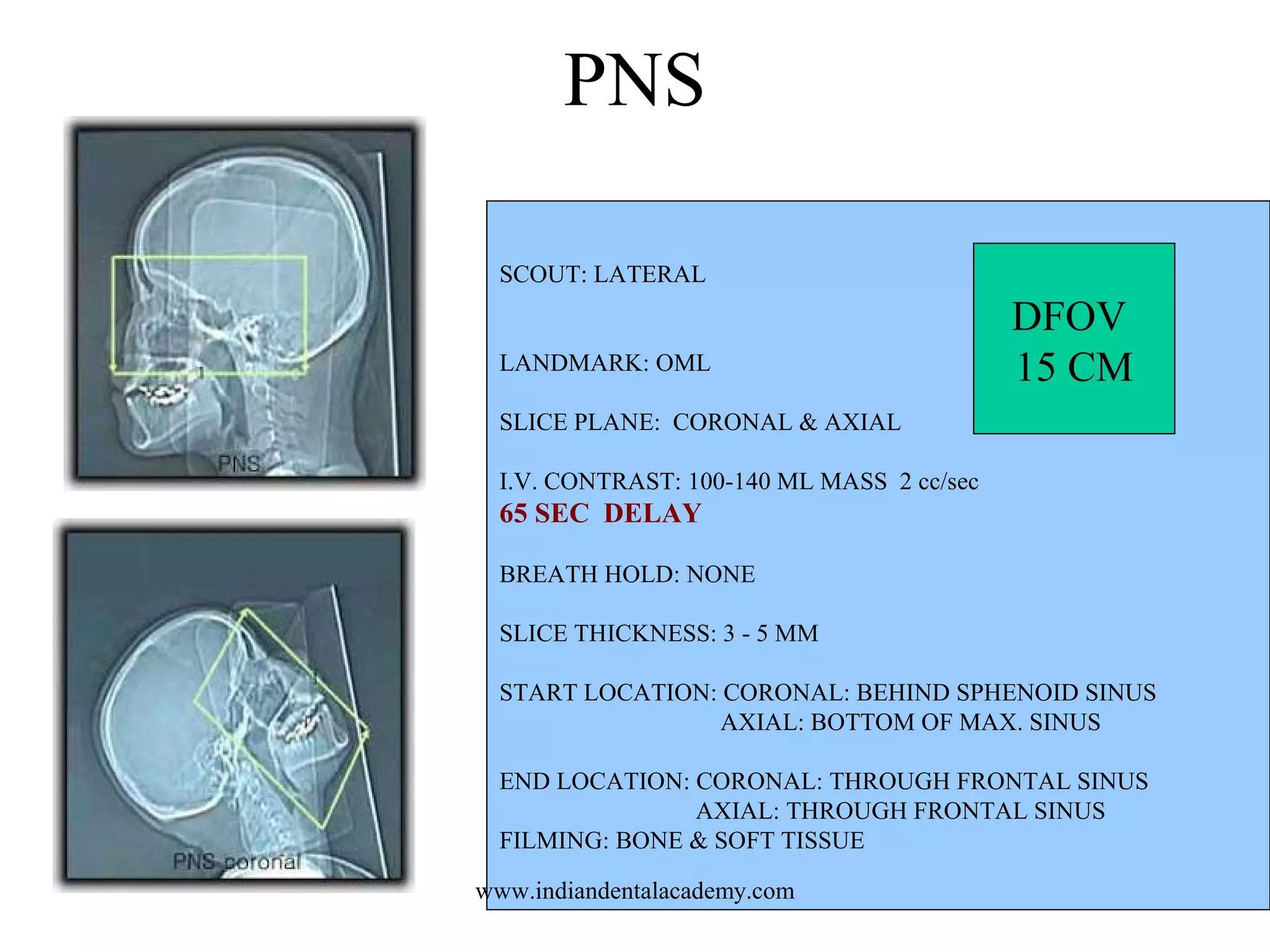
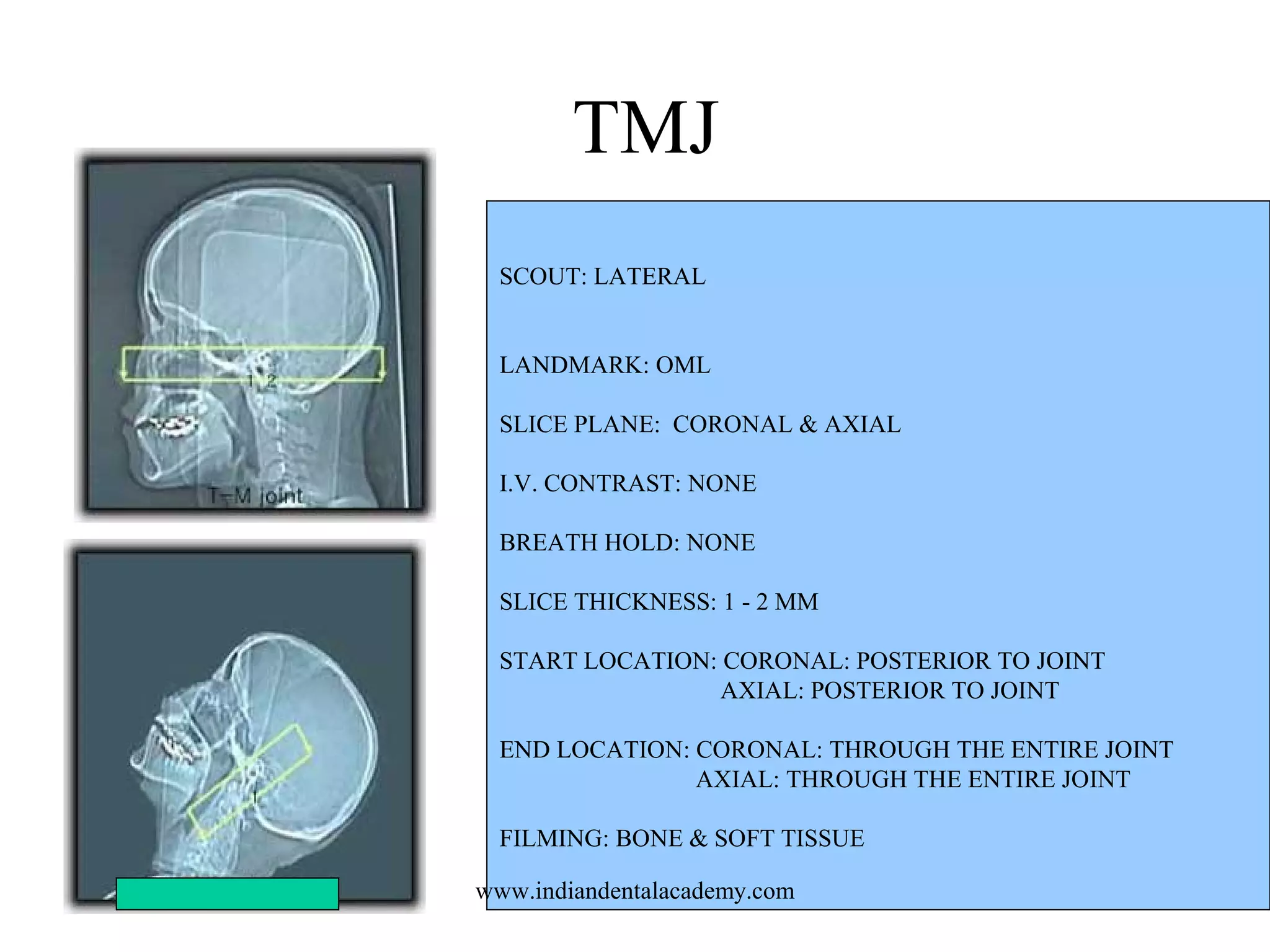
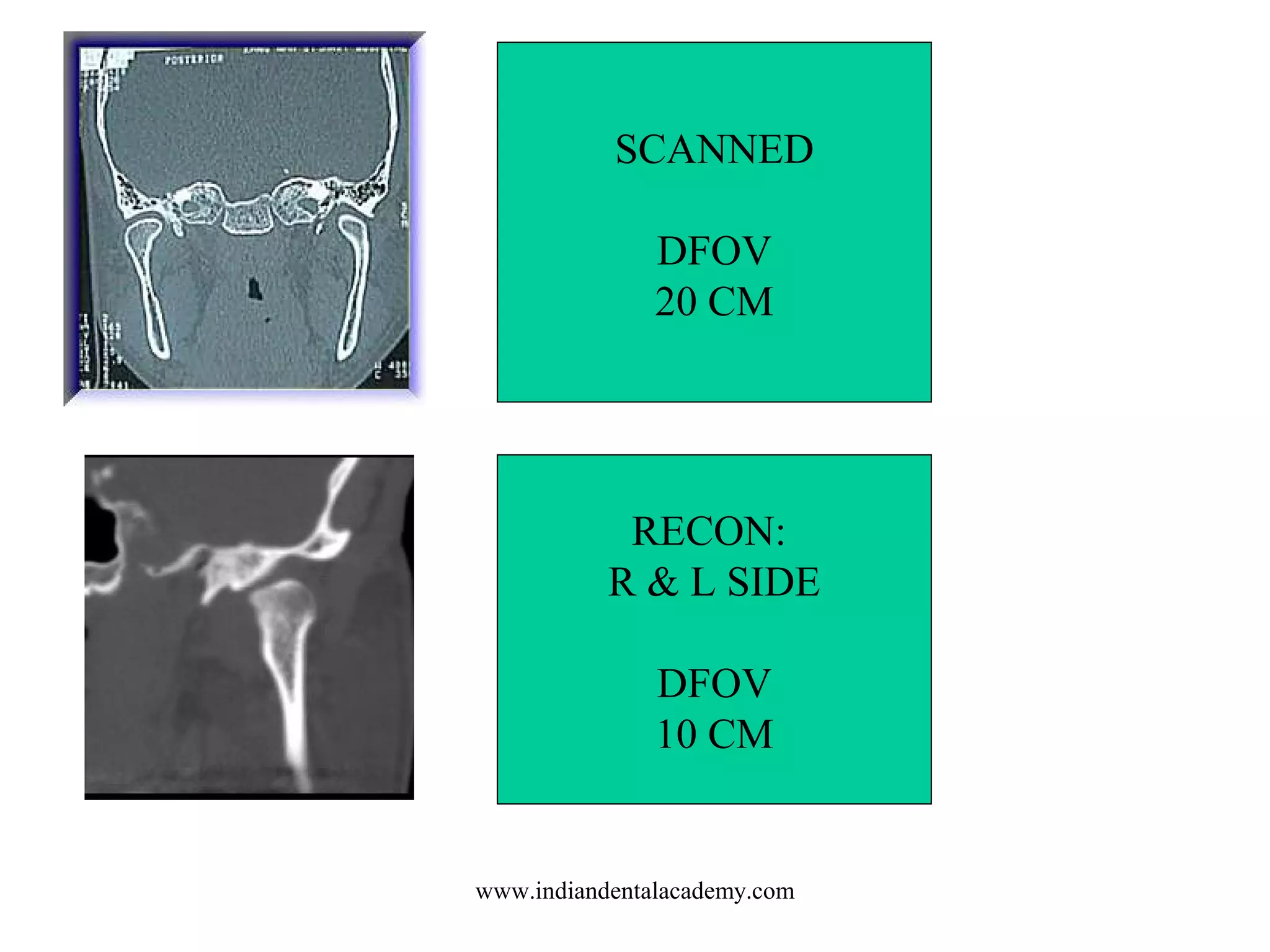


The document outlines various head pathologies and their corresponding protocols including sinusitis, skull fractures, brain tumors, and types of hemorrhages. It details specific conditions such as cerebral infarcts, brain infections, and arteriovenous malformations, and discusses imaging techniques like CT scans for diagnosis and treatment planning. Additionally, it provides protocols for imaging different areas of the head, emphasizing the importance of contrast and slice thickness in capturing detailed images.