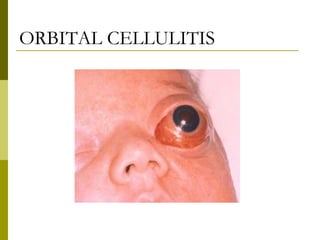
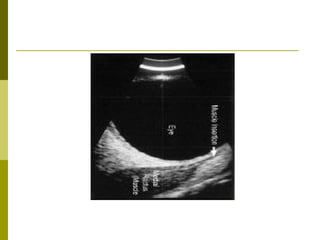
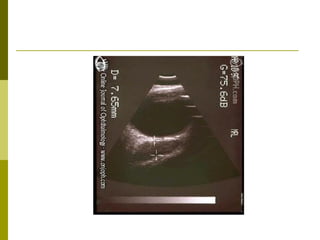
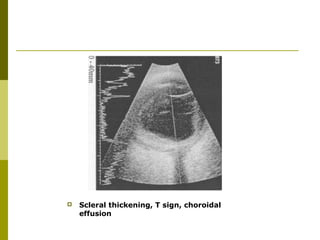
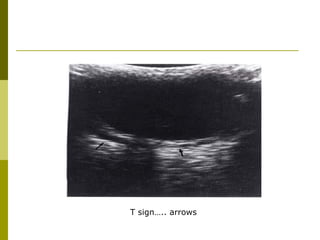
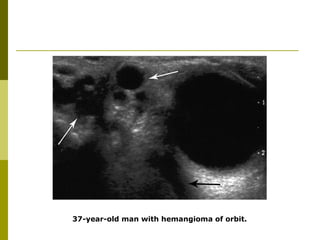
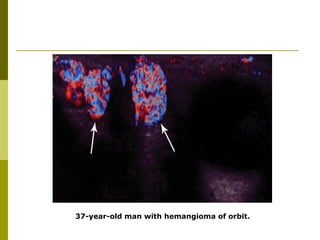
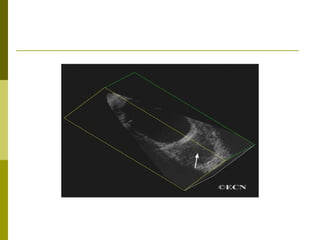
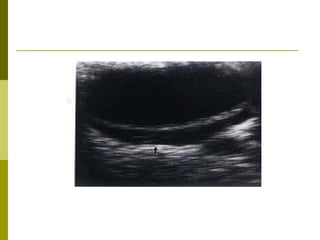
This document discusses the use of ultrasound in evaluating orbital pathologies. It outlines the advantages and disadvantages of ultrasound for orbital imaging. Key advantages include rapidity, accessibility, lack of radiation, ability to follow lesions over time, and lower cost compared to CT or MRI. Common orbital conditions seen in both children and adults are described, along with characteristic ultrasound findings for each condition. These include dermoid cysts, rhabdomyosarcoma, optic nerve glioma, thyroid ophthalmopathy, and others. Imaging features useful in diagnosis, such as lesion shape, borders, internal reflectivity, and Doppler flow, are emphasized. A variety of orbital masses, inflammatory conditions, and structural abnormalities are shown through ultrasound images.