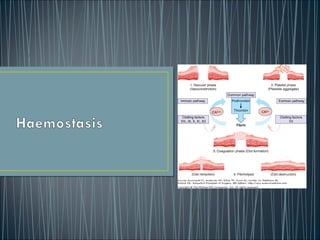
Haemostasis involves three key processes working together to stop bleeding from damaged blood vessels: primary haemostasis where platelets form a plug, secondary haemostasis where coagulation factors in the bloodstream form a clot, and fibrinolysis which breaks down clots once healing is complete. Platelets play a pivotal role in primary haemostasis by binding to collagen and von Willebrand factor at the site of injury and aggregating to form the initial platelet plug. The coagulation cascade then generates thrombin which converts fibrinogen to fibrin to strengthen the platelet plug. Fibrinolysis regulates haemostasis by breaking down fibrin over time as healing occurs.
Hemostasis and coagulation of blood For M.Sc & Basic Medical Students by Pand...Pandian M
Blood coagulation
Mechanism of coagulation
STAGES OF HEMOSTASIS
Coagulation of blood
Factors involved in blood clotting
Enzyme cascade theory
Mechanisms for formation of prothrombin activator
Fibrinolysis
Anticlotting mechanism in the body
Applied physiology
Hemostasis is the arrest of bleeding, whether it be by normal vasoconstriction (the vessel walls closing temporarily), by an abnormal obstruction (such as a plaque) or by coagulation or surgical means (such as ligation)
the objectives from this ppt :-
1.Define haemostasis.
2.Describe the main mechanisms that prevent blood loss after an injury.
3.Describe role of platelets in haemostasis.
4.Outline the mechanism of platelet plug formation.
5.Describe the mechanisms of blood coagulation.
Platelet and coagulation post graduate lecture Monkez M Yousif
This lecture is prepared for postgraduate students in Internal medicine. It presents a physiologic and basic background of the process of homeostasis followed by a practical approach to diagnosis and brief information of different causes of bleeding disorders
Hemostasis definition, types and steps.
Hemostasis and coagulation physiology and pathology in steps and illustrated in simple way by diagrams.
Intrinsic and extrinsic pathways are mentioned in details.
Platelet function as a corner stone hemostasis in case of endothelial injury or another pathology taht affect endothelium or blood vessels.
Some pharmacological notes about drugs related to hemostasis and its clinical significance.
Hemostasis and coagulation of blood For M.Sc & Basic Medical Students by Pand...Pandian M
Blood coagulation
Mechanism of coagulation
STAGES OF HEMOSTASIS
Coagulation of blood
Factors involved in blood clotting
Enzyme cascade theory
Mechanisms for formation of prothrombin activator
Fibrinolysis
Anticlotting mechanism in the body
Applied physiology
Hemostasis is the arrest of bleeding, whether it be by normal vasoconstriction (the vessel walls closing temporarily), by an abnormal obstruction (such as a plaque) or by coagulation or surgical means (such as ligation)
the objectives from this ppt :-
1.Define haemostasis.
2.Describe the main mechanisms that prevent blood loss after an injury.
3.Describe role of platelets in haemostasis.
4.Outline the mechanism of platelet plug formation.
5.Describe the mechanisms of blood coagulation.
Platelet and coagulation post graduate lecture Monkez M Yousif
This lecture is prepared for postgraduate students in Internal medicine. It presents a physiologic and basic background of the process of homeostasis followed by a practical approach to diagnosis and brief information of different causes of bleeding disorders
Hemostasis definition, types and steps.
Hemostasis and coagulation physiology and pathology in steps and illustrated in simple way by diagrams.
Intrinsic and extrinsic pathways are mentioned in details.
Platelet function as a corner stone hemostasis in case of endothelial injury or another pathology taht affect endothelium or blood vessels.
Some pharmacological notes about drugs related to hemostasis and its clinical significance.
Disseminated Intravascular coagulation is a very common and life endangering pathological condition due to consumptive coagulopathy.
This is a very serious disease and prompt diagnosis may help in early initiation of treatment.
Hemostasis is the mechanism that leads to cessation of bleeding from a blood vessel. It is a process that involves multiple interlinked steps. This cascade culminates into the formation of a “plug” that closes up the damaged site of the blood vessel controlling the bleeding.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
263778731218 Abortion Clinic /Pills In Harare ,sisternakatoto
263778731218 Abortion Clinic /Pills In Harare ,ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group of receptionists, nurses, and physicians have worked together as a teamof receptionists, nurses, and physicians have worked together as a team wwww.lisywomensclinic.co.za/
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...
Haemostasis and Bleeding Disorders
1.
2. • Haemostasis is the normal physiological response to
prevent significant blood loss following vascular injury
• Cellular and molecular mechanisms interact to seal
damaged blood vessels with localized clot formation to
prevent excessive blood loss
• Haemostasis consists of
-Primary haemostasis with vascular contraction and
platelet formation.
-Clotting of the plasma (secondary haemostasis)-
Involving interaction between numerous factors and
inhibitors
-Fibrinolysis- Process for removing the clot once blood
vessel’s integrity has been restored.
3. • Under normal circumstances blood
components pass unhindered through
the circulatory system
• The vascular barrier provides a non-
thrombotic surface due to the
production of platelet inhibitors
• In contrast, the subendothelial layer is
highly thrombogenic- contains collagen,
von Willebrand factor (VWF) and other
proteins that are involved in platelet
adhesion
• When the vascular endothelium is
disrupted, VWF is released, collagen is
exposed and tissue factor (TF) is
expressed on the surface of endothelial
cells.
• The vascular endothelium switches to a
prothrombotic state and 1° and 2°
haemostasis ensues.
4. • Plays a pivotal role in
primary haemostasis
• Alongside the vessel
wall and adhesive
proteins, forms the
initial ‘platelet plug’
• Activated platelets
express phospholipids
which promote localised
coagulation and the
generation of thrombin
and fibrin
5. • Ligand engagement of G1b/V/IX
by VWF/collagen in damaged
blood vessels activate platelets
• Activated plates changes from
discoid (2um) to irregular shape
with pseudopods, releasing its
granular content (FV, FVIII, Ca, 5-
HT, fibrinogen, ADP and
thromboxane).
• Platelet activation triggers
conformational changes in
GPIIb/IIIa from inactive state to
active state
• Fibrinogen and VWF function as
bridges between GPIIb/IIIa on
neighbouring activated platelets
• Activated platelets provide a
phospholipid domain, which
becomes a catalytic centre for
secondary haemostasis.
6. • Platelet’s integrin membrane glycoprotein IIb/IIIa increases its affinity to bind
fibrinogen.
• Fibrinogen crosslinks with glycoprotein IIa/IIIa supporting the aggregation of
adjacent platelets.
7.
8. • Results in the conversion of thrombin to fibrin,
strengthening the aggregated platelets (2°haemostasis)
• Damaged blood vessels expressing Tissue Factor [TF]
activates coagulation
• TF binds to circulating VIIa, forming the ‘Extrinsic tenase’
• In the presence of factor V, converts factor IX IXa and
factor XXa
• FXa then binds to prothrombin and generates a small
amount of fibrin.
• Thrombin generation through this reaction is not robust
and can be effectively terminated by TF pathway inhibitor
9. • Since the amount of
thrombin is insufficient
to convert fibrinogen
to fibrin, numerous
positive feedback
loops exists
• Thrombin generated
in the initiation phase
further activates FV
and VIII, which serves
as cofactors in its
propagation
10. • Continuous thrombin
generation is ensured
by the action of two
complexes: FVIIIa
complexed to FIXa
(intrinsic tenase), and
FVa to Xa
(prothrombinase).
• This occurs on the
surface of platelets and
leads to the appropriate
localization formation of
greater amounts of
thrombin.
11. The thrombin generated results in the formation of fibrin and activation of factor XIII (fibrin stabilizing
factor).
FXIII covalent links soluble fibrin monomers to form a stable polymer and provides strength and
stability to the fibrin incorporated into the platelet plug.
12. • Coagulation is regulated
and localized by several
anticoagulant
mechanisms.
• Most important includes
anti-thrombin, which
inhibits thrombin, and
factors IXa, Xa, XIa and
XIIa.
• Others include TF
Pathway inhibitor which
inhibits the TF-VIIa
complex and thrombin
• Activated Protein C, which
binds to thrombomodulin
and cleaves FVa and
FVIIIa.
13. • Fibrinolysis is activated at
the same time that the
coagulation system but
operates more slowly and is
important for the regulation
of haemostasis.
• In the presence of fibrin,
tissue plasminogen activator
(tPA) cleaves plasminogen,
producing plasmin which
proteolyzes fibrin.
• Result in the protein
fragment D-dimer, a fibrin
degradation product which is
a useful marker of
fibrinolysis.
14. Haemophilia A and B
• Haemphilia A and B and the two most common forms of
severe inherited bleeding disease.
• Both conditions are X-linked recessive
• Majority affected individuals are males
• 20% of female carriers of haemophilia can also express a
mild bleeding tendency (variation pattern of X
inactivation)
• Diagnosis made through a combination of clinical and
laboratory features.
• ~60% of cases will have a family history of the condition
15. Haemophilia A and B
• Clinical manifestations are very similar for factor VIII
deficiency (haemophilia A), and factor IX deficiency
(haemophilia B)
• Severe disease (factor levels <1%) results in frequent
episodes of spontaneous musculoskeletal bleeding
• Moderate severe disease (factor levels 1-5%) usually do
not manifest spontaneous bleeding
• Mild haemophilia (factor levels 5-40%) only bleed on
provocation
• Current treatment involves various forms of protein
replacement therapy
16. Haemophilia A and B
• Schematic showing the intrinsic and extrinsic pathways of the
coagulation cascade leading to fibrin formation. A deficiency or
dysfunction of coagulation factorVIII orfactorIXcompromises the
activation of factorX, the ensuing reactions are inefficient and
haemophilia results.
17. Von Willebrands Disease
• Most common inherited bleeding disorder of humans
• Prevalence symptomatic subjects of ~1 in 1000
• Females outnumber males by 2:1 presumably due to
manifesting excessive mucocutaneous bleeding at the
time on menses and childbirth
• 3 types- Type 1 disease is a quantitative deficiency of
functionally normal VWF (~65% of VWD cases)
Type 2 VWD represents a group of qualitative
VWF variants (types 2A, 2B, 2M and 2N)
comprising approximately 30% of VWD
Type 3 VWD is the virtual absence of VWF
(~1 in 1 million of the population )
19. Diagnosis of VWD
• Diagnosis requires consideration of 3 components-
personal history of excessive mucocutaneous bleeding,
lab. test consistent with VWD, and a family history of
VWD.
• Many cases of Type 1 and some type 2 cases can be
treated with desmopressin
• Remaining cases require transfusion with plasma
deprived VWF-FVIII concentrates.
21. Haemostasis in LiverImpairment
• Liver is involved in the synthesis of most clotting factor proteins
• In liver impairment, clotting factor proteins are reduced with the
exception of FVIII.
• Decreased capacity to clear activated clotting factor-inhibitor
complexes.
• Liver failure also result in reduced platelet count and function.
• These defects are counterbalanced by a concomitant defect in
anticoagulant and pro-fibrinolytic factors.
• Decreased in platelet function is counterbalanced by elevated levels
of Von Willebrand factor.
• This rebalance is represented by limited bleeding during surgery.
• Coagulopathy in patients with critical liver dysfunction is complex
and quickly decompensate to bleeding as well and thrombosis.