Downloaded 24 times
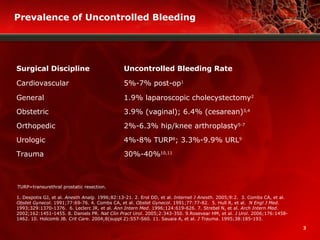
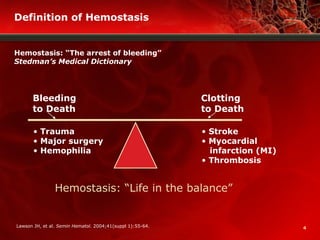
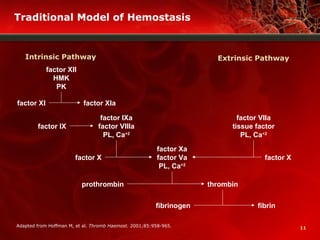
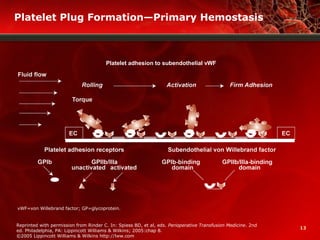

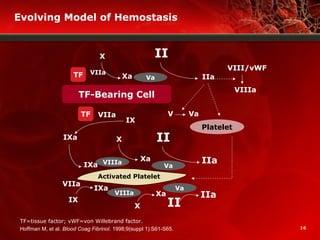
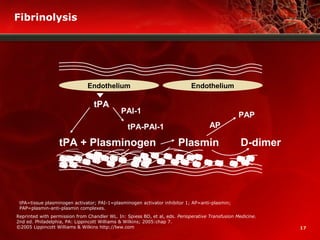

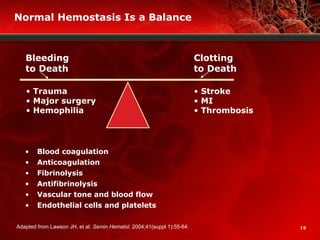
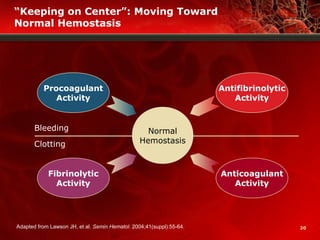
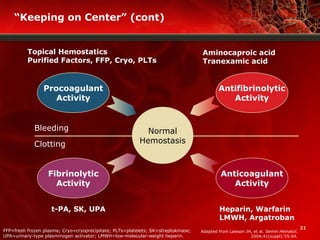
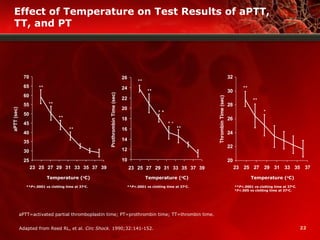

The document discusses the physiology of hemostasis, including: - The essential components of hemostasis including platelet plug formation, coagulation pathways, and fibrinolysis. - Conditions that can increase the risk of uncontrolled bleeding during surgery such as patient comorbidities, anticoagulant medications, hypothermia and acidosis. - How achieving optimal hemostasis requires balancing procoagulant, anticoagulant, fibrinolytic and antifibrinolytic factors.























































































