CONTENTS
. Introduction
. Definition
.Classification
. Causes Of Haemorrhage
. Clinical Features
. Hematological Features
. Haemostasis
. Stages Of Haemostasis
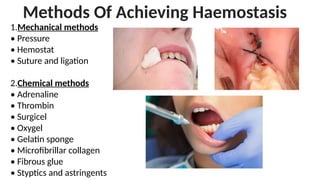
. Methods Of Achieving Haemostasis
. Wound Healing
. Healing Of Extraction Socket
. Complications
. Recent Advances
. Conclusion
. Reference
3.
INTRODUCTION
• Haemorrhage canoccur a greater or lesser degree during all surgical
procedures. Major hemorrhages are common among patients with
bleeding/clotting disorders or those who are on anti coagulants.
4.
DEFINITION
• Haemorrhage denotesthe escape of blood from the cardiovascular
system to the surface of body or into its tissues or cavities.
5.
CLASSIFICATION
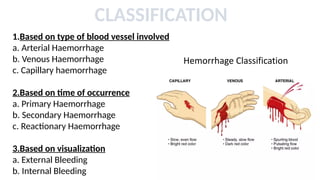
1.Based on typeof blood vessel involved
a. Arterial Haemorrhage
b. Venous Haemorrhage
c. Capillary haemorrhage
2.Based on time of occurrence
a. Primary Haemorrhage
b. Secondary Haemorrhage
c. Reactionary Haemorrhage
3.Based on visualization
a. External Bleeding
b. Internal Bleeding
6.
4.Based on volumeof blood loss
a. Mild Haemorrhage
b. Moderate Haemorrhage
c. Severe Haemorrhage
5.Based on speed of blood loss
a. Acute Haemorrhage
b. Chronic Haemorrhage
6.Based on percentage of blood loss
a. Class 1
b. Class 2
c. Class 3
d. Class 4
7.
Primary Haemorrhage
• Occursat the time of injury
• Body attempt to stop the bleeding by clot formation.
Secondary Haemorrhage
• Primary bleeding has stopped and wound start to bleed again after 24
hours and may continue for days.
• It may occur due to:
Dislodgement of clot
Secondary trauma to the wound
Infections
8.
Reactionary Haemorrhage
• Reactionarybleeding occurs within 8 hours after stoppage of primary
bleeding
• Caused due to loose foreign bodies in the wound like calculus,broken
bone piece,dislodgement of clot.
9.
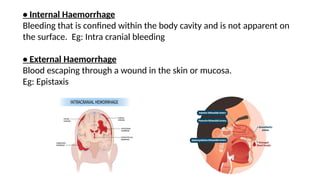
• Internal Haemorrhage
Bleedingthat is confined within the body cavity and is not apparent on
the surface. Eg: Intra cranial bleeding
• External Haemorrhage
Blood escaping through a wound in the skin or mucosa.
Eg: Epistaxis
• Increased pulserate
• Increased pallor
• Restlessness
• Air hunger
• Thirst
• Cold clammy skin
• Tinnitus "ringing in the ears"
• Blindness
• Reduced urinary output
CLINICAL FEATURES
12.
HAEMATOLOGICAL INVESTIGATIONS
Majority ofdefects of hemostasis can be screened by these
basic tests:
• Bleeding time
• Platelet count
• Prothrombin time
• Partial thromboplastin time
• Thrombin time
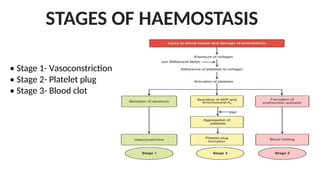
Vasoconstriction
• Damage tothe blood vessel causes narrowing of the lumen to limit the
blood loss.
• Local factors involved :
Thromboxane A2
Serotonin
Fibrinopeptide B
17.
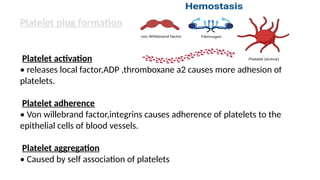
Platelet plug formation
Plateletactivation
• releases local factor,ADP ,thromboxane a2 causes more adhesion of
platelets.
Platelet adherence
• Von willebrand factor,integrins causes adherence of platelets to the
epithelial cells of blood vessels.
Platelet aggregation
• Caused by self association of platelets
Management Of SecondaryHaemorrhage In
Normal Patients
• This management occurs a few days after surgery,it involves the removal of
any debris from the wound surface.
• Identify the source of bleeding and treat as would be done in a patient with
secondary bleeding.
• Surgical stents can be placed over sockets for stabilization of clot and
prevention of wound contamination.
23.
Management Of HaemorrhageIn Patients With
Bleeding Disorders/Those On Anti Coagulant Therapy
• Pre-operative blood investigations should be carried out,pre-operative
correction of the underlying deficiency(replacement of clotting factors or
platelets).
• After this appropriate local measures to be carried out to decrease the
chances of post- operative bleeding.
24.
Management Of HaemorrhageIn Patients
With Uncontrolled Hypertension
• Prior appropriate medical consultation to decrease blood pressure.
• Once blood pressure is controlled,then bleeding decreases and with
local measures the hemorrhage is controlled.
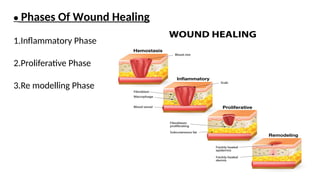
Inflammatory Phase
• Beginswhen wound develops.
• Lasts 4 to 6 days immune system works to prevent microbial colonization.
• Marked by oedema,erythema,pain and inflammation.
28.
Proliferative Phase
• Lastsanother 4-24 days.
• Granulation tissue fills in the wound.
• Fibroblasts lay collagen in the wound bed.
• Wound edges begin to contract.
• Epithelial cells migrate from wound margins.
29.
Re modelling Phase
•Lasts for several years.
• Collagenous matrix forms a scar after continuous remodelling.
• Stronger type 1 collagen replaces type 3.
• Any disruption during the phase leads to formation of exuberant scar
or wound dehiscence.
30.
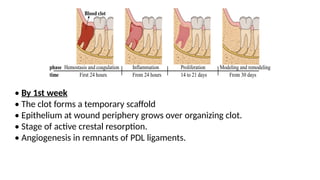
HEALING OF ANEXTRACTION SOCKET
• Healing by second intention.
• Blood fills extraction site after removal of tooth from socket.
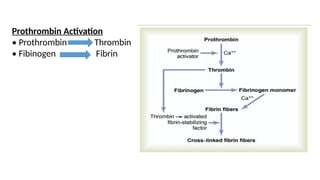
• Both intrinsic and extrinsic pathways of clotting cascade are activated.
• Resultant fibrin meshwork containing entrapped RBCs seals off the torn
blood vessels and reduces the size of the extraction wound.
• Organization of clot begins within the first 24 to 48 hrs with dilation of blood
vessels,leucocyte migration and formation of a fibrin layer
31.
• By 1stweek
• The clot forms a temporary scaffold
• Epithelium at wound periphery grows over organizing clot.
• Stage of active crestal resorption.
• Angiogenesis in remnants of PDL ligaments.
32.
By 2nd week
•Clot continues to get organized through fibroplasia.
• New blood vessels migrate to center of the clot.
By 3rd week
• Extraction socket filled by granulation tissue
• Surface of wound completely re epithelialized with minimal or no
scar formation.
RECENT ADVANCES
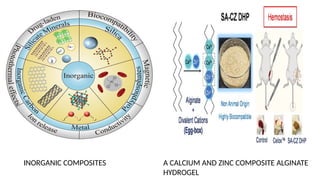
•Application andprogress of inorganic composites in haemostasis: (April 2024)
This review focuses on the haemostatic mechanisms of silicate minerals (zeolite,
montmorillonite, and bioglass), silica (mesoporous silica and diatomaceous
silica), polyphosphates, inorganic carbon materials (graphene and carbon
nanotubes), metal-containing materials (metal–organic frameworks) and related
composite haemostatic materials.
In recent years, inorganic composite haemostatic materials have received
widespread attention for their ability to rapidly stop bleeding and for their low
biotoxicity.
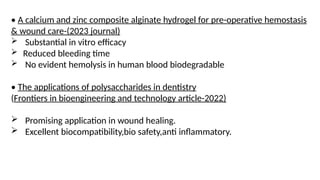
• A calciumand zinc composite alginate hydrogel for pre-operative hemostasis
& wound care-(2023 journal)
Substantial in vitro efficacy
Reduced bleeding time
No evident hemolysis in human blood biodegradable
• The applications of polysaccharides in dentistry
(Frontiers in bioengineering and technology article-2022)
Promising application in wound healing.
Excellent biocompatibility,bio safety,anti inflammatory.
37.
• A studynamed Assessment and comparison of the hemostatic efficacy
of ferrum phosphoricum against other conventional methods in minor
oral sugical procedures-International journal of applied dental
sciences(2021)
Found that ferrum content helps balance iron & oxygen in
blood,phosphorous prevents bleeding.
Shorten bleeding time,better healing.
38.
• Topical andeffective hemostatic medicines in the battlefield(2015)
Uncontrolled hemorrhage has been considered as one of the most
important factors for causing death on the battlefront
If given timely and efficient hemostatic medicines in pre-hospital setting,
patients will obtain more time and chance to wait for medical treatment so
as to save their lives.
The hemostatic materials Hemcon and QickClot are widely used in the battle
and proved to be the most effective ways to stop bleeding. However, as new
agents get to emerge and the side effects of those well-known efficient
devices have been exposed gradually, people start to doubt the efficacy of
them. So Fibrin Sealant dressing, Celox and Woundstat are more effective
to stanch hemorrhage than others.
40.
CONCLUSION
Control of haemorhageis the most important part of any surgical procedure.
The main step in prevention of hemorrhage in dental clinic is detailed history
taking of the patient,adequate precaution of apprehensive patient as
haemorrhages require medical attention and can be deadly.
41.
REFERENCE
• Textbook ofOral and Maxillofacial Surgey by S M Balaji
• Textbook of Oral and Maxillofacial Surgery by Neelima Anil Mallik
• Peterson’s Principles of Oral and Maxillofacial Surgery
• International journal of applied dental sciences

![• Trauma
• Infection
• Local irritants
• Congenital malformations
• Surgical
• Haemophilia
• Liver disease
• Urinary infection
• Systemic diseases
• Abnormalities in clotting factors [eg :Haemophilia A]
• Abnormalities in platelets [eg :ITP]
CAUSES OF HAEMORRHAGE](https://image.slidesharecdn.com/haemorrhage-250615053404-45ef3b0a/85/HAEMORRHAGE-power-point-presentationnnnn-10-320.jpg)