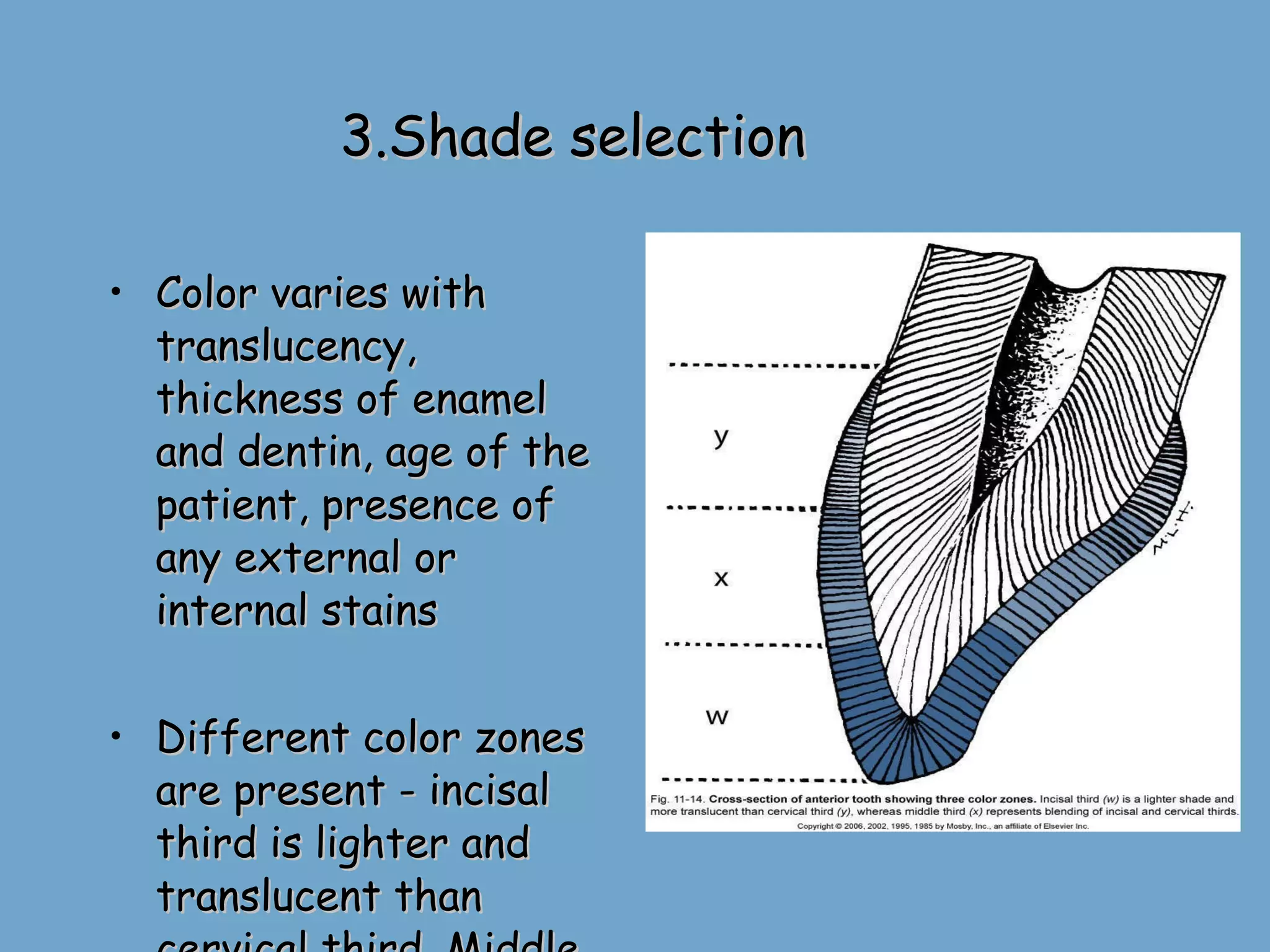
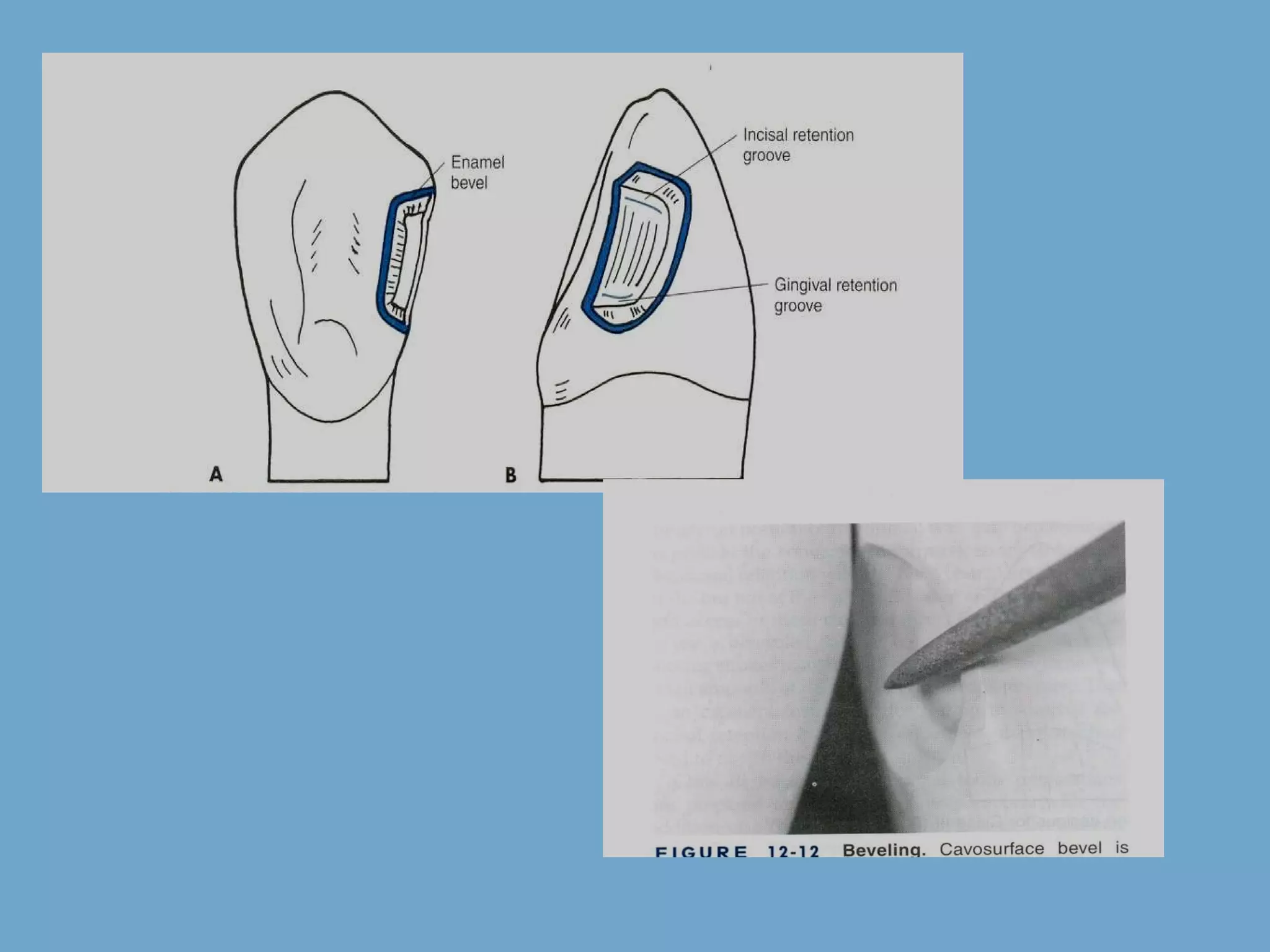
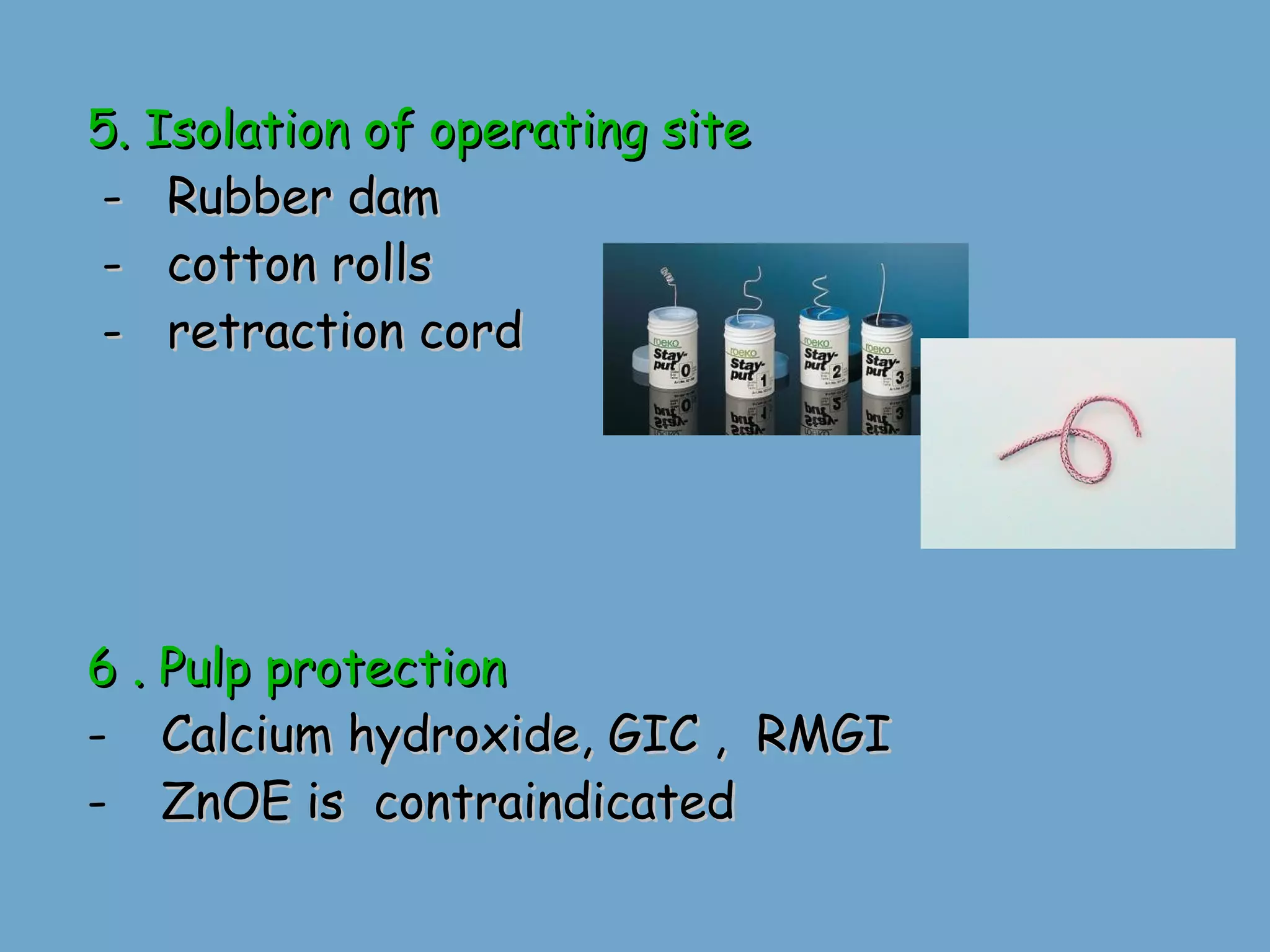
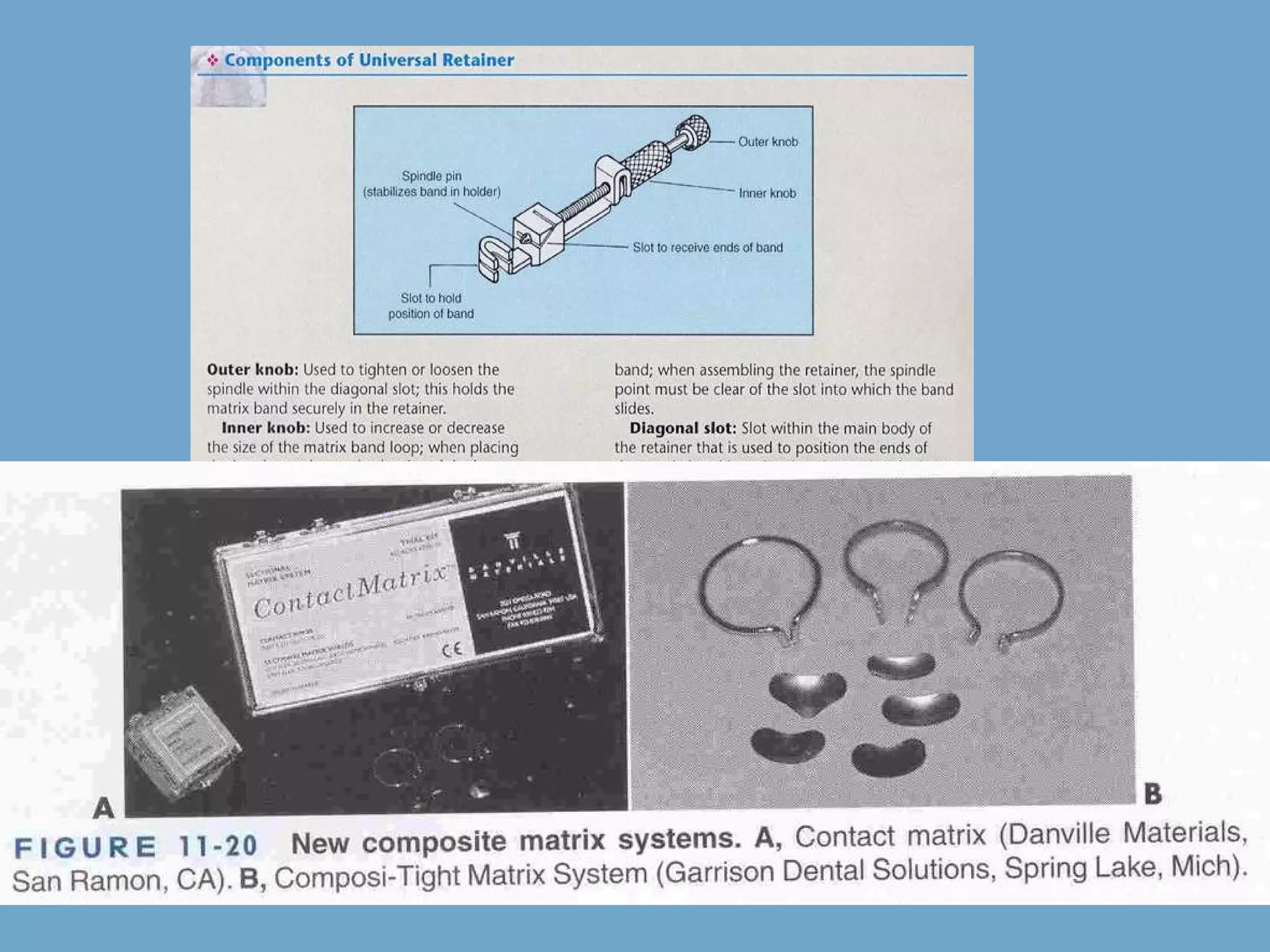
The document discusses the clinical technique for composite restoration. It covers initial procedures like local anesthesia and shade selection. It then discusses tooth preparation, including cavity designs like conventional, beveled conventional, modified box shape, and facial/lingual slot. Matrix placement and isolation of the operating site are also covered. Pulp protection and restorative techniques are briefly mentioned.